Efficacy
IKEMA Trial Results
44 MONTHS FOLLOW-UP1
SARCLISA + Kd demonstrated an unprecedented mPFS of 3 years1-23
Median follow-up of 44 months for an anti-CD38 treatment in a pivotal trial that includes lenalidomide-refractory patients1
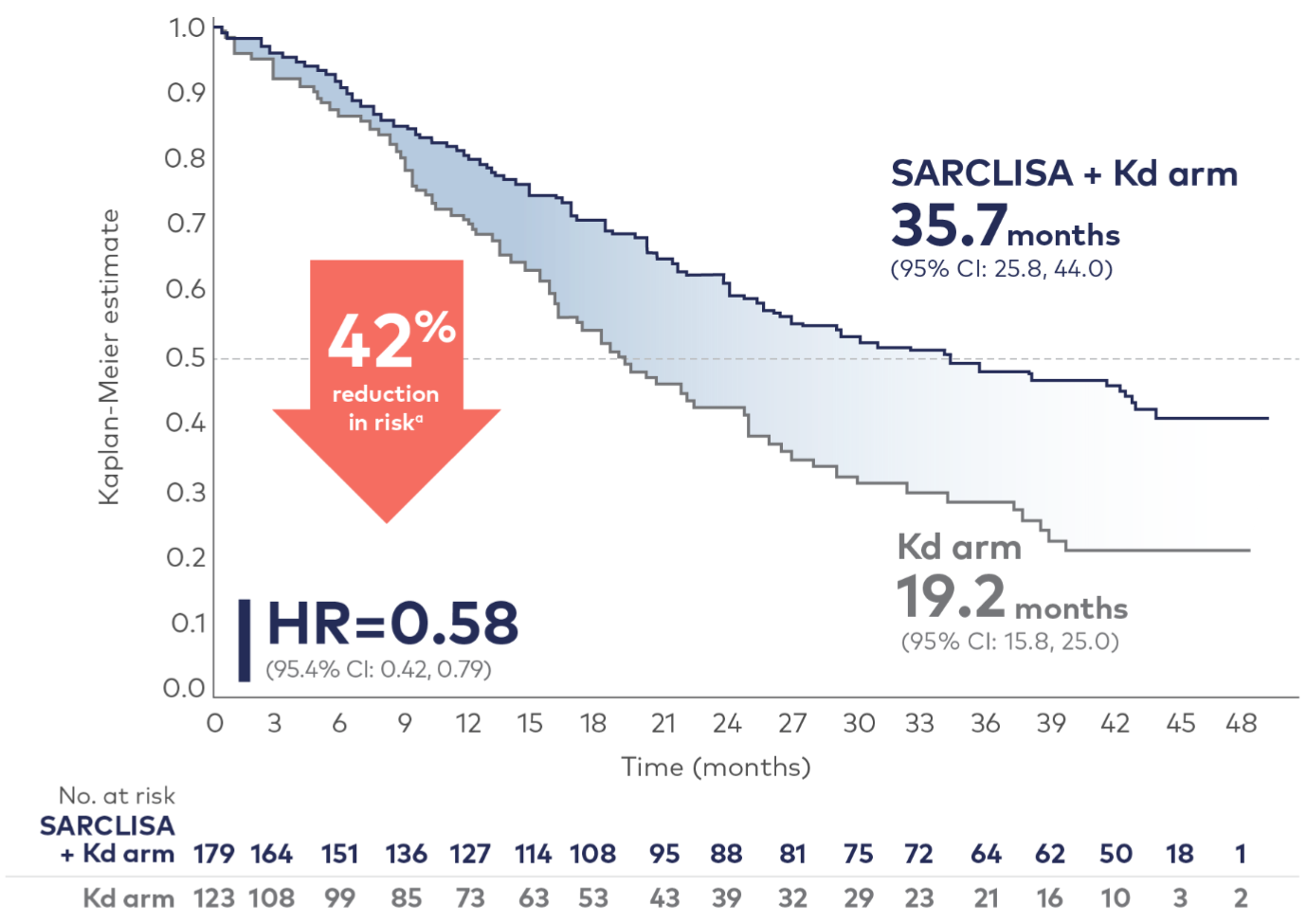
PFS results were assessed by an IRC, based on central laboratory data for M-protein, and central radiologic imaging review using the IMWG criteria.2
aReduction in risk of death or progression.2
HR=hazard ratio; IMWG=International Myeloma Working Group; IRC=independent response committee; Kd=carfilzomib and dexamethasone; mPFS=median progression-free survival; NDMM=newly diagnosed multiple myeloma; NR=not reached; RRMM=relapsed and/or refractory multiple myeloma.
References: 1. Martin T, Dimopoulos MA, Mikhael J, et al. Isatuximab, carfilzomib, and dexamethasone in patients with relapsed multiple myeloma: updated results from IKEMA, a randomized phase 3 study. Blood Cancer J. 2023;13(1):72. doi:10.1038/s41408-023-00797-8 2. SARCLISA [summary of product characteristics]. sanofi-aventis groupe: Paris, France; 2025. 3. Hernández-Rivas JÁ, Ríos-Tamayo R, Encinas C, Alonso R, Lahuerta JJ. The changing landscape of relapsed and/or refractory multiple myeloma (MM): fundamentals and controversies. Biomark Res. 2022;10(1):1-23. 4. Spicka I, Ocio EM, Oakervee HE, et al. Randomized phase III study (ADMYRE) of plitidepsin in combination with dexamethasone vs. dexamethasone alone in patients with relapsed/refractory multiple myeloma. Ann Hematol. 2019;98(9):2139-2150. 5. Usmani SZ, Quach H, Mateos MV, et al. Carfilzomib, dexamethasone, and daratumumab versus carfilzomib and dexamethasone for patients with relapsed or refractory multiple myeloma (CANDOR): updated outcomes from a randomised, multicentre, open-label, phase 3 study. Lancet Oncol. 2022;23(1):65-76. 6. Schjesvold FH, Dimopoulos MA, Delimpasi S, et al. Melflufen or pomalidomide plus dexamethasone for patients with multiple myeloma refractory to lenalidomide (OCEAN): a randomised, head-to-head, open-label, phase 3 study. Lancet Haematol. 2022;9(2):e98-e110. doi:10.1016/S2352-3026(21)00381-1 7. Du J, Fang B, Li J, et al. A study of carfilzomib and dexamethasone in patients with relapsed and refractory multiple myeloma in China. Int J Hematol. 2021;113(3):422-429. 8. Terpos E, Gobbi M, Potamianou A, Lahaye M, Couturier C, Cavo M. Retreatment and prolonged therapy with subcutaneous bortezomib in patients with relapsed multiple myeloma: a randomized, controlled, phase III study. Eur J Haematol. 2018;100(1):10-19. 9. Dimopoulos M, Siegel DS, Lonial S, et al. Vorinostat or placebo in combination with bortezomib in patients with multiple myeloma (VANTAGE 088): a multicentre, randomised, double-blind study. Lancet Oncol. 2013;14(11):1129-1140. 10. Dimopoulos MA, Palumbo A, Corradini P, et al. Safety and efficacy of pomalidomide plus low-dose dexamethasone in STRATUS (MM-010): a phase 3b study in refractory multiple myeloma. Blood. 2016;128(4):497-503. 11. Usmani SZ, Nahi H, Legiec W, et al. Final analysis of the phase III non-inferiority COLUMBA study of subcutaneous versus intravenous daratumumab in patients with relapsed or refractory multiple myeloma. Haematologica. 2022;107(10):2408-2417. 12. Study to evaluate the safety and efficacy of pomalidomide monotherapy in subjects with refractory or relapsed refractory multiple myeloma. ClinicalTrials.gov identifier: NCT01324947. Updated November 19, 2019. Accessed June 16, 2022. https://clinicaltrials.gov/ct2/show/NCT01324947 13. Janssen Research & Development. Final synoptic clinical study report: report of long-term extension. A phase 3, randomized, open-label study of subcutaneous and intravenous VELCADE® in combination with dexamethasone in Chinese subjects with relapsed or refractory multiple myeloma. Protocol 26866138MMY3037; Phase 3 JNJ-26866138-AAA (bortezomib). Published April 23, 2019. Accessed June 6, 2022. 14. Hájek R, Masszi T, Petrucci MT, et al. A randomized phase III study of carfilzomib vs low-dose corticosteroids with optional cyclophosphamide in relapsed and refractory multiple myeloma (FOCUS). Leukemia. 2017;31(1):107-114. 15. Kropff M, Baylon HG, Hillengass J, et al. Thalidomide versus dexamethasone for the treatment of relapsed and/or refractory multiple myeloma: results from OPTIMUM, a randomized trial. Haematologica. 2012;97(5):784-791. 16. Hjorth M, Hjertner Ø, Knudsen LM, et al. Thalidomide and dexamethasone vs. bortezomib and dexamethasone for melphalan refractory myeloma: a randomized study. Eur J Haematol. 2012;88(6):485-496. 17. Usmani SZ, Nahi H, Plesner T, et al. Daratumumab monotherapy in patients with heavily pretreated relapsed or refractory multiple myeloma: final results from the phase 2 GEN501 and SIRIUS trials. Lancet Haematol. 2020;7(6):e447-e455. doi:10.1016/S2352-3026(20)30081-8 18. Lonial S, Lee HC, Badros A, et al. Belantamab mafodotin for relapsed or refractory multiple myeloma (DREAMM-2): a two-arm, randomised, open-label, phase 2 study. Lancet Oncol. 2020;21(2):207-221. 19. Bahlis NJ, Dimopoulos MA, White DJ, et al. Daratumumab plus lenalidomide and dexamethasone in relapsed/refractory multiple myeloma: extended follow-up of POLLUX, a randomized, open-label, phase 3 study. Leukemia. 2020;34(7):1875-1884. 20. GSK provides update on DREAMM-3 phase III trial for Blenrep in relapsed/refractory multiple myeloma. Press release. London, United Kingdom: GSK; November 7, 2022. https://www.gsk.com/en-gb/media/press-releases/gsk-provides-update-on-dreamm-3-phase-iii-trial-for-blenrep/ 21. Fu W, Li W, Hu J, et al. Daratumumab, bortezomib, and dexamethasone versus bortezomib and dexamethasone in Chinese patients with relapsed or refractory multiple myeloma: updated analysis of LEPUS. Clin Lymphoma Myeloma Leuk. 2023;23(1):e51-e58. doi:10.1016/j.clml.2022.10.007 22. Moreau P, Garfall AL, van de Donk NWCJ, et al. Teclistamab in relapsed or refractory multiple myeloma. N Engl J Med. 2022;387(6):495-505. 23. Rodriguez‑Otero P, Ailawadhi S, Arnulf B, et al. Ide-cel or standard regimens in relapsed and refractory multiple myeloma. N Engl J Med. 2023;388(11):1002-1014.
Sanofi does not recommend the use of its products in any manner inconsistent with that described in the label available in your country. Please refer to your local product labelling information before prescribing.
Name and Presentation: SARCLISA 20 mg/mL concentrate for solution for infusion. Each vial contains 100 mg of isatuximab in 5 mL of concentrate (100 mg/5 mL) or 500 mg of isatuximab in 25 mL of concentrate (500 mg/25 mL). Isatuximab is an immunoglobulin G1 (IgG1) monoclonal antibody (mAb).
Therapeutic indications: In combination with pomalidomide and dexamethasone, for the treatment of adult patients with relapsed and refractory multiple myeloma (MM) who have received at least two prior therapies including lenalidomide and a proteasome inhibitor (PI) and have demonstrated disease progression on the last therapy. In combination with carfilzomib and dexamethasone, for the treatment of adult patients with multiple myeloma who have received at least one prior therapy. In combination with bortezomib, lenalidomide, and dexamethasone, for the treatment of adult patients with newly diagnosed multiple myeloma who are ineligible for autologous stem cell transplant.
Pediatric population: Outside its authorised indications, SARCLISA has been studied in children aged 28 days to less than 18 years of age with relapsed or refractory acute lymphoblastic or myeloid leukaemia but efficacy has not been established.
Dosage and administration: SARCLISA should be administered by a healthcare professional, in an environment where resuscitation facilities are available. Premedication should be used 15-60 minutes prior to SARCLISA infusion with the following medicinal products to reduce the risk and severity of infusion reactions: Dexamethasone 40 mg (when administered in combination with isatuximab and pomalidomide) or 20 mg (when administered in combination with isatuximab and carfilzomib; or when administered in combination with isatuximab, bortezomib, and lenalidomide) oral or intravenous, 20 mg for patients ≥75 years of age, Acetaminophen, Diphenhydramine, H2 antagonists. The recommended dose of SARCLISA is 10 mg/kg body weight administered as an intravenous infusion in combination with pomalidomide and dexamethasone or in combination with carfilzomib and dexamethasone or in combination with bortezomib, lenalidomide, and dexamethasone (isatuximab regimen). Dosing schedule in combination with pomalidomide and dexamethasone or in combination with carfilzomib and dexamethasone: cycle 1: days 1, 8, 15 and 22 (weekly), cycle 2 and beyond: days 1, 15 (every 2 weeks). Each treatment cycle consists of a 28-day period. Dosing schedule in combination with bortezomib, lenalidomide, and dexamethasone: cycle 1: days 1, 8, 15, 22 and 29, cycles 2 to 4: days 1, 15 and 29 (every 2 weeks), cycles 5 to 17: days 1 and 15 (every 2 weeks), cycles 18 and beyond: day 1 (every 4 weeks). Each treatment cycle consists of a 42-day period from cycle 1 to 4, and of a 28-day period from cycle 5. Treatment is repeated until disease progression or unacceptable toxicity.
Method of administration: SARCLISA is for intravenous use. For details on preparation and infusion rate see full SmPC.
Contraindications: Hypersensitivity to the active substance or to any of the excipients. See full SmPC for full list of excipients.
Warnings and precautions: Infusion reactions, mostly mild or moderate, were observed in 38.2% of patients treated with SARCLISA in ICARIA, and in 45.8% in IKEMA but resolved on the same day in 98% of infusions, and in 24.0% of patients treated with Isa-VRd in IMROZ and resolved the same day in 97.3% of patients. The most common symptoms of an IR included dyspnoea and chills. The most common severe sign and symptom was hypertension. Vital signs should be frequently monitored during the entire infusion and when required infusion should be interrupted or permanently discontinued in case symptoms that do not improve to grade ≤1 after infusion interruption. Serious infusion reactions including severe anaphylactic reactions have also been observed after SARCLISA administration. Most of the grade 3-4 neutropenia was reported as laboratory abnormalities. In patients treated with Isa-VRd, neutropenia was reported as a laboratory abnormality in 87.5% of patients and as an adverse reaction in 30% of patients. Neutropenic complications have been observed in 1/3 of patients treated with SARCLISA. A higher incidence of infections including grade ≥3 infections occurred with SARCLISA. Antibacterial and antiviral prophylaxis (such as herpes zoster prophylaxis) according to treatment guidelines should be considered during treatment. Patients receiving SARCLISA should be closely monitored for signs of infection. Physicians should carefully evaluate patients before and during treatment as per International Myeloma Working Group (IMWG) guidelines for occurrence of secondary primary malignancies (SPM) and treatment should be initiated as indicated. Patients should be monitored closely, and appropriate precautions taken for tumor lysis syndrome. Isatuximab binds to CD38 on red blood cells (RBCs) and may result in a false positive indirect antiglobulin test (indirect Coombs test). This interference with the indirect Coombs test may persist for at least 6 months after the last infusion of SARCLISA. Patient should have blood type and screen tests performed prior to the first infusion of Isatuximab and should be monitored for theoretical risk of haemolysis. For details in tests interference see full SmPC.
Drug interactions: Isatuximab has no impact on the pharmacokinetics of pomalidomide or carfilzomib, or bortezomib, or lenalidomide and vice versa. Isatuximab may interfere with serological testing and with Serum Protein Electrophoresis and Immunofixation assays. In patients with persistent very good partial response, where isatuximab interference is suspected, consider using a validated isatuximab-specific IFE assay to distinguish isatuximab from any remaining endogenous M protein in the patient’s, to facilitate determination of complete response.
Fertility, pregnancy and lactation: Women of childbearing potential treated with isatuximab should use effective contraception during treatment and for 5 months after cessation of treatment. The use of isatuximab in pregnant women is not recommended since there are no available data.
Undesirable effects: Observed in patients treated with isatuximab in combination with pomalidomide and dexamethasone: Infections/infestations: very common: pneumonia, upper respiratory tract infection, bronchitis: common: Herpes zoster. Neoplasms benign, malignant and unspecified: common: skin cancer, solid tumour (non-skin cancer): uncommon: haematology malignancy. Blood/lymphatic system disorders: very common: neutropenia, thrombocytopenia, common: febrile neutropenia, anaemia, unknown frequency: lymphopenia. Metabolism and nutrition disorders: very common: decreased appetite. Cardiac disorders: common: atrial fibrillation. Respiratory, thoracic and mediastinal disorders: very common: dyspnoea. Gastrointestinal disorders: very common: diarrhoea, nausea, vomiting. Investigations: common: weight decreased. Injury, poisoning and procedural complications: very common: infusion reaction. Immune system disorders: uncommon: anaphylactic reaction. Observed in patients treated with isatuximab in combination with carfilzomib and dexamethasone: Infections/infestations: very common: pneumonia, upper respiratory tract infection, bronchitis: common: Herpes Zoster. Vascular disorder: very common: hypertension. Neoplasms benign, malignant and unspecified: common: Skin cancers and solid tumors non-skin cancers. Blood/lymphatic system disorders: common: neutropenia, anaemia, thrombocytopenia, unknown frequency: lymphopenia. Respiratory, thoracic and mediastinal disorders: very common: dyspnoea and cough. Gastrointestinal disorders: very common: diarrhoea and vomiting. General disorders and administration site conditions: very common: Fatigue. Injury, poisoning and procedural complications: very common: infusion reaction. Immune system disorders: uncommon: anaphylactic reaction. Reported in patients with multiple myeloma treated with isatuximab in combination with bortezomib, lenalidomide, and dexamethasone: Infections/infestations: very common: pneumonia, bronchitis, Covid-19. Neoplasms benign, malignant and unspecified: common: skin cancer, solid tumour, uncommon: haematology malignancy. Blood and lymphatic system disorders: very common: neutropenia, thrombocytopenia, common: anaemia, not known: lymphopenia. Immune system disorders: uncommon: anaphylactic reaction. Eye disorders: very common: cataract. Gastrointestinal disorders: very common: diarrhoea, common: vomiting. General disorders and administration site conditions: very common: fatigue. Injury, poisoning and procedural complications: very common: infusion reaction.
Pharmacotherapeutic group: Antineoplastic agents, monoclonal antibodies, ATC code: L01FC02.
List of excipients: Sucrose, Histidine hydrochloride monohydrate, Histidine, Polysorbate 80 and Water for injections.
Legal classification: Prescription Only Medicine.
Marketing authorization holder: Sanofi Winthrop Industrie, 82, avenue Raspail, 94250 Gentilly, France.
Date of last revised: March 2025.
Abbreviated Prescribing Information based on the EU SmPC as of February 2025.
Before prescribing always refer to your full local prescribing information as this information may vary from country to country
MAT-GLB-2101917-v10.0-03/2025