- Article
- Source: Campus Sanofi
- Aug 8, 2025
Understanding an ITP Diagnosis

Immune thrombocytopenia (ITP) is an autoimmune disorder caused by complex immune dysregulation, leading to a reduction in platelet count. It is difficult to diagnose because there is no conclusive test for the condition.1,2 This article covers the diagnostic criteria for immune thrombocytopenia, differential diagnoses, and lab tests that may be involved in a typical ITP workup.
ITP diagnosis: from idiopathic thrombocytopenic purpura to immune thrombocytopenia
Previously, the abbreviation “ITP” referred to idiopathic thrombocytopenic purpura. However, as the understanding of the condition grew, it was found that the pathogenesis of ITP involved the production of autoantibodies against platelet glycoproteins. In addition, not all patients presented with purpura at the time of diagnosis. Therefore, the abbreviation ITP now stands for immune thrombocytopenia to more accurately reflect the disease.1
Currently, there is no “gold standard” test that can diagnose immune thrombocytopenia. ITP diagnosis is often made by excluding other causes of isolated thrombocytopenia using methods such as evaluation of patient history, blood count, and evaluation of peripheral blood film.2
Diagnostic criteria for ITP
Primary ITP is typically defined as a platelet count of less than 100x109/L (100,000/μL) with no evidence of leucopenia or anaemia, and when all other causes of thrombocytopenia—such as certain drugs, liver diseases, or pseudothrombocytopenia—have been ruled out.1,2 Patients with ITP can be asymptomatic despite low platelet counts, but the risk of bleeding appears to increase when platelets drop below 20 x 109/L.1,2
Diagnosing primary vs secondary ITP
Immune thrombocytopenia can be categorised into primary and secondary ITP depending on the cause of the condition3:
- Secondary ITP: This form of immune thrombocytopenia occurs due to an inciting factor. This can be a drug, an infection such as H. pylori, or other malignancies. The ITP differential diagnosis process often involves testing for these causes.4
- Primary ITP: When all possible causes of secondary immune thrombocytopenia are ruled out, the patient is diagnosed with primary ITP. The cause here can be idiopathic or autoimmune-system mediated.4
Differential diagnosis
The differential diagnosis workup for immune thrombocytopenia involves testing for conditions with symptoms that may overlap with ITP. 3
|
Differential diagnoses of thrombocytopenia include3:
|
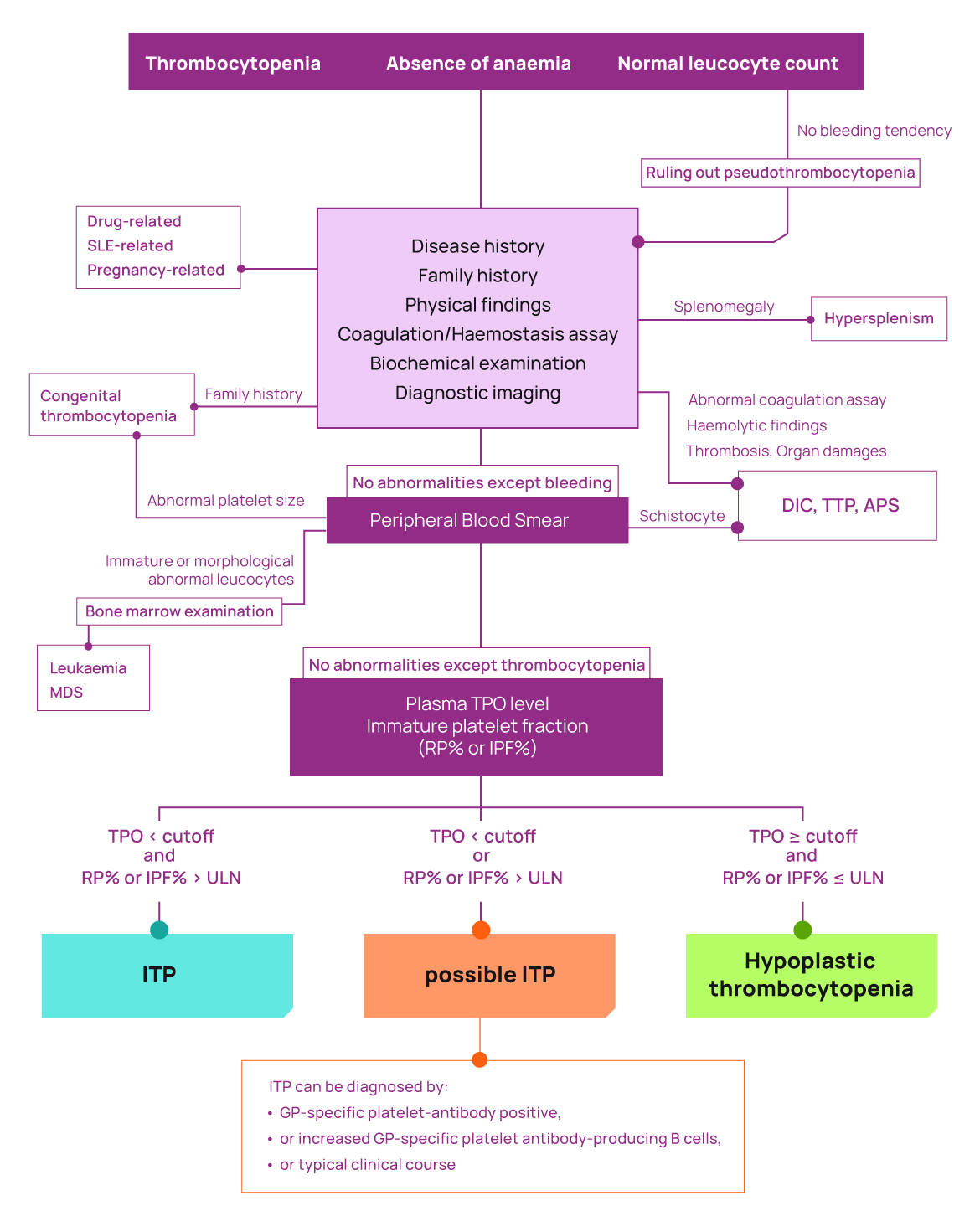
Adapted from Kashiwagi H, et al. Int J Hematol. 2024;119(1):1-13.5
Diagnosing acute, chronic, and persistent ITP
Immune thrombocytopenia can be further categorised into acute, chronic, and persistent forms depending on the duration of disease. Some classifications and guidelines also consider newly diagnosed ITP and severe ITP as distinct forms.6,7
- Acute ITP: Also known as short-term ITP, this refers to ITP where symptoms resolve in 12 months or less.6,7
- Newly diagnosed ITP: Patients with ITP diagnosed in the past 3 months are said to have newly diagnosed ITP.6,7
- Persistent ITP: Patients diagnosed with ITP in the past 3-to-12 months, who have not reached spontaneous remission, or are not maintaining a complete response off-therapy, are said to have persistent ITP.6,7
- Chronic ITP: ITP is termed as chronic when the disease persists for 12 months or more.6,7
- Severe ITP: Severe ITP is characterised by bleeding at presentation at levels sufficient to mandate treatment. Severe ITP may also necessitate the use of a new platelet-enhancing therapy or an increased dose of current treatment to control symptoms.6,7
Tests used in an immune thrombocytopenia workup
As ITP is diagnosed based on medical history and a process of exclusion, every diagnosis journey looks different.4
Typical factors used to inform an immune thrombocytopenia diagnosis include1,4:
- Medical history: Analysis of personal history with a focus on drugs and medical conditions that have the potential to cause thrombocytopenia.
- Family history: ITP is generally not an inherited disorder, so a family history of thrombocytopenia or other bleeding disorders can indicate another, possibly inherited cause of thrombocytopenia.
- Physical exam: Presence of conditions like lymphadenopathy or hepatosplenomegaly may suggest other underlying causes of thrombocytopenia. Children with ITP are usually well-appearing except for bruising symptoms associated with thrombocytopenia, while two-thirds of adults show a wide range of bleeding symptoms.
The exact lab workup varies due to the individualised nature of ITP differential diagnosis; however, some of the lab tests that can be used are listed below.1,4
Blood tests
The first step in ITP diagnosis is the determination of isolated thrombocytopenia. The defining feature of thrombocytopenia is a low platelet count (below 150,000/μL), which can be determined through a complete blood count, and a blood smear.8
- Complete Blood Count (CBC): CBC is used to measure the level of platelets in the blood.8
- Blood smear: The presence of giant platelets in a blood smear, caused by increased platelet turnover and release of immature forms into circulation can indicate immune thrombocytopenia.8
Ultrasound
Ultrasound can be used to assess the size of the spleen, to exclude splenomegaly as the cause of thrombocytopenia. The presence of fatty liver and splenomegaly may indicate a diagnosis other than immune thrombocytopenia.9
Coombs test and quantitative immunoglobulin analysis
A direct antiglobulin test (DAT), or direct Coombs Test, is used to analyse the presence of antibodies circulating around red blood cells (RBCs) that can induce haemolysis. It can also be used to determine the safety of immunoglobulin therapy and other immune-modifying treatments. Studies show that a positive DAT has a known association with chronic ITP.10,11
Screening for thrombocytopenia-associated infections
Some bacterial and viral infections can induce thrombocytopenia or secondary immune thrombocytopenia. Screening for these infections can help rule out primary immune thrombocytopenia. Some of these infections include4:
- HIV
- Hepatitis C
- Helicobacter pylori
- Epstein-Barr virus
Bone marrow biopsy
Bone marrow biopsies can be used to distinguish between immune thrombocytopenia and other haematological malignancies. However, they are not commonly used in children and adults unless clinical examination suggests the presence of conditions such as neutropenia, leucocytosis, or bone marrow failure. Bone marrow analysis is also recommended if the patient is unresponsive to immunotherapy.4
Thrombopoietin (TPO) tests
In people with ITP, thrombopoietin levels are normal or slightly elevated. In some cases, measuring thrombopoietin levels can be helpful to distinguish between immune thrombocytopenia and hypoplastic thrombocytopenia.5
Considering ITP treatment options
While platelet levels are useful in diagnosing ITP, they are not the only factor governing bleeding symptoms and management. Studies show that people with similar platelet levels do not necessarily show the same incidence of bleeding symptoms.12,13
As such, ITP treatment decisions should consider more than just platelet levels. Beyond bleeding, ITP can increase risk of thrombosis and has numerous effects on patients’ lives, including fatigue, anxiety, depression, and headaches. Patients with chronic ITP may become so accustomed to a life with reduced quality of life, that they believe it is their “normal.”14
A holistic understanding of the disease and the patient is required for their treatment. Options that act on the immune dysregulation in ITP can potentially benefit patients.15
APS, antiphospholipid syndrome; CVID, common variable immune deficiency; DIC, disseminated intravascular coagulation; GP, platelet glycoprotein; HIV, human immunodeficiency virus; HUS, hemolytic-euremic syndrome; IPF, immature platelet fraction; MDS, myelodysplastic syndrome; PD-1, programmed cell death 1; RP, reticulated platelets; SLE, systemic lupus erythematosus; TAR, thrombocytopenia-absent radius; TPO, thrombopoietin; TTP, thrombotic thrombocytopenia purpura; ULN, upper limit of normal.
References
1. McCrae K. Immune thrombocytopenia: no longer “idiopathic.” Cleve Clin J Med. 2011;78(6):358-373. 2. Gafter-Gvili A. Current approaches for the diagnosis and management of immune thrombocytopenia. Eur J Intern Med. 2023;108:18-24. 3. Provan D, Arnold DM, Bussel JB, et al. Updated international consensus report on the investigation and management of primary immune thrombocytopenia. Blood Adv. 2019;3(22):3780-3817. 4. Pietras NM, Gupta N, Justiz Vaillant AA, Pearson-Shaver AL. Immune Thrombocytopenia. In: StatPearls. Treasure Island (FL): StatPearls Publishing; May 5, 2024. 5. Kashiwagi H, Kuwana M, Murata M, et al. Reference guide for the diagnosis of adult primary immune thrombocytopenia, 2023 edition. Int J Hematol. 2024;119(1):1-13. 6. Rodeghiero F, Stasi R, Gernsheimer T, et al. Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children: report from an international working group. Blood. 2009;113(11):2386-2393. 7. National Heart, Lung, and Blood Institute. Platelet Disorders - Immune Thrombocytopenia (ITP). National Institutes of Health. Updated July 24, 2025. Accessed April 9, 2026. https://www.nhlbi.nih.gov/health/immune-thrombocytopenia 8. Gauer RL, Braun MM. Thrombocytopenia. Am Fam Physician. 2012;85(6):612-622. https://www.aafp.org/pubs/afp/issues/2012/0315/p612.html 9. Kelton JG, Vrbensky JR, Arnold DM. How do we diagnose immune thrombocytopenia in 2018? Hematology Am Soc Hematol Educ Program. 2018;2018(1):561-567. 10. Theis SR, Hashmi MF. Coombs Test. In: StatPearls. StatPearls Publishing; September 12, 2022. 11. Kim TO, Grimes AB, Kirk S, et al. Association of a positive direct antiglobulin test with chronic immune thrombocytopenia and use of second line therapies in children: a multi-institutional review. Am J Hematol. 2019;94(4):461-466. 12. Frelinger AL III, Grace RF, Gerrits AJ, et al. Platelet function tests, independent of platelet count, are associated with bleeding severity in ITP. Blood. 2015;126(7):873-879. 13. Rodeghiero F, Michel M, Gernsheimer T, et al. Standardization of bleeding assessment in immune thrombocytopenia: report from the International Working Group. Blood. 2013;121(14):2596-2606. 14. Cooper N, Kruse A, Kruse C, et al. Immune thrombocytopenia (ITP) World Impact Survey (iWISh): patient and physician perceptions of diagnosis, signs and symptoms, and treatment. Am J Hematol. 2021;96(2):188-198. 15. Kim DS. Recent advances in treatments of adult immune thrombocytopenia. Blood Res. 2022;57(S1):112-119.
MAT-GLB-2500852-v2.0-05/2026