
Beyfortus® (nirsevimab-alip) has been studied across multiple infant cohorts, including healthy, preterm, and at-risk infants, with consistent efficacy and safety data demonstrated in clinical trials. This page highlights key study designs, RSV hospitalization outcomes, and emerging real-world evidence.1
Beyfortus® (nirsevimab-alip) 50 mg and 100 mg Injection has been evaluated in real-world settings in2:
400K+
|
50+
|
9
|
4
|
*In Andorra, Australia, Chile, France, Italy, Luxembourg, Portugal, Spain, and the United States as of August 5, 2025.2
Pivotal trials
In 2 randomized, placebo-controlled pivotal trials, Beyfortus demonstrated efficacy against MA RSV-LRTI and RSV hospitalization.1,3-5*
In Trial 04, Beyfortus exhibited a reduction in MA RSV hospitalization compared to placebo: healthy term and late preterm infants (≥35 wGA)1,3-5
Trial 04 Primary Cohort†‡§

Trial 04 full study cohort1‡

In Trial 03, Beyfortus exhibited a reduction in MA RSV-LRTI and RSV hospitalization compared to placebo: healthy preterm infants (≥29 to <35 wGA)1,6
Trial 03||¶

Trial 03 post hoc analysis1,7#

Signs of LRTI involvement included rhonchi, rales, crackles, or wheezing, and at least one sign of worsening clinical severity, including at least one of the following: increased respiratory rate, hypoxemia, acute hypoxic or ventilatory failure, new-onset apnea, nasal flaring, retractions, grunting, or dehydration due to respiratory distress.1
CI, confidence interval; IM, intramuscular; MA RSV-LRTI, medically attended respiratory syncytial virus lower respiratory tract infection; RRR, relative risk reduction; wGA, weeks gestational age.
*Results of Trials 04 and 03 for infants entering their first RSV season.1
†Primary Cohort: 1,490 healthy term and late preterm infants (≥35 wGA) in Trial 04.1
‡During Trial 04, the COVID-19 pandemic interrupted trial enrollment. The efficacy analysis is based on the Primary Cohort, which included those participants enrolled prior to the pause due to COVID-19. Trial 04 continued monitoring the Primary Cohort and included an additional 1,522 subjects enrolled after the pause to comprise the full study cohort. The full study cohort included 3,012 infants randomized to receive Beyfortus or placebo in the post hoc analysis.4
§Efficacy for MA RSV-LRTI is based on RRR against placebo, adjusted for age at randomization.1
||1,453 preterm infants (≥29 to <35 wGA) in Trial 03.1
¶Efficacy for MA RSV-LRTI is based on RRR against placebo, adjusted for age at randomization and hemisphere.1
#860 infants from the full study cohort of 1,453 healthy preterm infants in Trial 03 were analyzed in a post hoc analysis. For infants in their first RSV season, the recommended dose is 50 mg for infants <5 kg or 100 mg for infants ≥5 kg via IM injection.1,7
Most common adverse reactions in Trial 04 and Trial 03 were rash (0.9%) and injection site reactions (0.3%)1*
Trial 04 and Trial 03 were pooled to evaluate the safety of Beyfortus (N=2,570) compared to placebo (N=1,284).1
- Adverse reactions were reported in 1.2% of infants who received Beyfortus; most (97%) adverse reactions were mild to moderate in severity
*The Safety Population includes all infants who received the recommended dose of Beyfortus in Trials 04 and 03: Primary and Safety cohorts from Trial 04; infants who weighed <5 kg and who received the recommended dose of Beyfortus (single 50 mg IM dose) in Trial 03.1
Summary of real-world evidence study summaries8-15
Real-world evidence study |
Date |
Endpoints |
| NIRSE-GAL
Galicia, Spain | From September 25, 2023, to March 31, 20248 | Effectiveness and population health impact of Beyfortus against RSV-LRTI hospitalization8,9*† |
| NIRSE-CL
Chile | Between April 1, 2024, and September 30, 2024 (seasonal group); Between October 1, 2023, and March 31, 2024 (catch-up group)10 | Effectiveness and population health impact of Beyfortus against RSV-LRTI hospitalization10‡ |
| EPI-PHARE
France | 2024-2025 RSV season11 | Hospitalization for RSV-associated LRTI11 |
| HARMONIE
France, Germany, and the United Kingdom | First RSV season for infants in France, Germany, or the United Kingdom ending on February 28, 2023, in each country12 |
Primary endpoint:
Secondary endpoint:
|
| BEAR
Kaiser Permanente Northern California (KPNC), US | 2023-2024 RSV season14 |
Co-primary endpoints14:
Post hoc analysis14:
|
| CDC real-world data
The New Vaccine Surveillance Network (NVSN), US | 2023-2024 RSV season15 | Overall incidence of MA RSV ARI and RSV hospitalization15 |
ARI, acute respiratory illness; BEAR, Beyfortus Effectiveness Against Medically Attended RSV Events in Infants; CDC, Centers for Disease Control and Prevention; EPI-PHARE, French National Agency for Medicines and Health Products Safety and French National Health Insurance; PCR, polymerase chain reaction.
*RSV hospitalization was defined as hospitalization for RSV-related LRTI. Effectiveness was estimated only using the catch-up group.8,9
†Nosocomial RSV infections were excluded from the study analysis.8
‡RSV hospitalization was defined as hospitalization for RSV-related LRTI.10
§Infants could be born before or during the RSV season, which began on September 11, 2022 (Week 37) in France; on October 9, 2022 (Week 41) in Germany; and on September 4, 2022 (Week 36) in the United Kingdom.12
‖Overall incidence of hospitalization for RSV-LRTI was defined as admission to the hospital on the basis of the treating physician’s decision and confirmation of RSV by means of a positive result of a test performed in accordance with routine practice, during the RSV season in France, Germany, and the United Kingdom.12
¶The characteristics of infants at randomization were similar in the 2 groups, and 85.2% of infants were ≥37 wGA at birth.12
#An episode is defined as having at least 1 LRTI-associated encounter in any setting in the 7 days before and up to 10 days after a positive RSV PCR test.14
**Each medical encounter was categorized as outpatient, emergency department, inpatient, or intensive care unit.14
††Episodes that included at least 1 hospitalization were considered a hospitalized RSV-LRTI.14
NIRSE-GAL
Effectiveness and impact of universal prophylaxis with Beyfortus in infants against hospitalization for RSV disease: results of a population-based longitudinal study in Galicia, Spain.16
Effectiveness of population-wide administration of Beyfortus on infant RSV hospitalization9,16
Infants aged <6 months eligible for Beyfortus immunization in Galicia, Spain, were analyzed in the NIRSE-GAL study. The 2023-2024 immunization campaign ran from September 25, 2023, to March 31, 2024. The population eligible to receive Beyfortus during the data collection period consisted of 3 groups: born during the season (infants born during the immunization campaign), born before the season (infants younger than 6 months at the start of the campaign), and a high-risk group. The high-risk group was not included in this analysis due to small sample size and low number of events.8*
Receipt of Beyfortus8
- Infants born before the season received electronic appointments to be immunized in their reference hospitals†
- Infants born during the season were offered Beyfortus immunization on the first day of life before being discharged†
Number of subjects and Beyfortus immunization coverage9
- Total infants immunized with Beyfortus (% [n/N]): 92.0% (13,320/14,476)
- Infants born before the season immunized with Beyfortus (% [n/N]): 88.5% (6,249/7,062)†
- Infants born during the season immunized with Beyfortus (% [n/N]): 95.3% (7,071/7,414)†
Key assessment: Effectiveness and population health impact of Beyfortus against RSV-LRTI hospitalization.8,9‡§
Baseline characteristics: Among the overall cohort of 14,476 infants, 12,950 were ≥37 wGA and 931 were <37 wGA. A total of 595 infants had missing wGA data.16
Safety was routinely monitored by the Galician pharmacovigilance system.16‖
Beyfortus implementation and effectiveness9

Safety results: No severe AEs directly related to Beyfortus were registered.9
Because Beyfortus coverage exceeded 90% in the seasonal cohort, and when combining the catch-up and seasonal cohorts, immunization effectiveness from Cox regression models was estimated only from the catch-up cohort.9
The NIRSE-GAL study is ongoing with a planned follow-up of 36 months.8
Population health impact of Beyfortus on RSV hospitalization9,16

No serious AEs directly linked to Beyfortus were reported.8,9‖
RSV-LRTI hospitalization after Beyfortus implementation16

AE, adverse event; CI, confidence interval; IQR, interquartile range; ITT, intention-to-treat; LRTI, lower respiratory tract infection; RSV, respiratory syncytial virus; wGA, weeks gestational age.
*Infants born during the season were born between September 25, 2023, and March 31, 2024. Infants born before the season were born between April 1, 2023, and September 24, 2023.8
†In the NIRSE-GAL study, infants born during the season were labeled “seasonal group” and infants born before the season were labeled “catch-up group.”8
‡RSV hospitalization was defined as hospitalization for RSV-related LRTI. Effectiveness was estimated only using the catch-up group.8,9
§Nosocomial RSV infections were excluded from the study analysis.8
‖AEs related to Beyfortus administration were routinely monitored through the Galician pharmacovigilance system. In addition, active surveillance of any potential AE or hospitalization in the first 3 weeks after Beyfortus administration was conducted in the preterm population (infants with a GA <37 weeks).8
¶In the ITT analysis, there were 24 RSV hospitalizations among a total of 6,249 immunized infants and 15 RSV hospitalizations among a total of 813 nonimmunized infants.9,16
#RSV hospitalization was defined as hospitalization for RSV-related LRTI. Effectiveness was estimated only using the ITT cohort.8,9
**Estimated by comparing events against historical data since 2016, excluding RSV seasons spanning the COVID-19 pandemic (2020-2022).8,9
NIRSE-CL
Effectiveness and impact of Beyfortus in Chile during the first season of a national immunization strategy against RSV (NIRSE-CL): a retrospective observational study.10
A national RSV prophylaxis strategy with Beyfortus in Chile targeted infants born between April 1, 2024, and September 30, 2024 (seasonal group); infants born between October 1, 2023, and March 31, 2024 (catch-up group); and a high-risk group. The high-risk group was not included in this analysis because identifying infants at high risk who were born before October 1, 2023, was not possible with the data that were available.10*
Receipt of Beyfortus10
- Infants born before the season: Parents or guardians were invited to bring infants to immunization centers through a national communications campaign
- Infants born during the season: Beyfortus immunization was offered before hospital discharge
Number of subjects and Beyfortus immunization coverage10
- Total infants immunized with Beyfortus (% [n/N]): 94.1% (145,087/154,173)†
- Infants born before the season immunized with Beyfortus (% [n/N]): 91.2% (72,246/79,183)†
- Infants born during the season immunized with Beyfortus (% [n/N]): 97.1% (72,841/74,990)†
Key assessment: Effectiveness and population health impact of Beyfortus against RSV-LRTI hospitalization.10‡
Baseline characteristics: Overall, 90.3% of infants were ≥37 wGA and 9.7% were <37 wGA.10
Beyfortus implementation and effectiveness10

Safety results: There were no pronounced safety events associated with the use of Beyfortus, and none of the 18 reported AEs supposedly attributable to immunization were directly attributed to the monoclonal antibody.10
The findings in this report are subject to limitations10:
- Testing for RSV is not routine practice throughout Chile; RSV was inferred as a cause of hospitalization using ICD-10 codes that were selected based on historical data from hospitals that routinely test for RSV
- The immunization status of approximately 2,300 infants could not be determined, and thus they were excluded from the primary analysis
- The counterfactual scenario constructed to estimate the impact of universal RSV prophylaxis with Beyfortus was based on circulation of RSV in recent years (2019, 2022, and 2023) and assumed no other strategy, such as one based on maternal vaccination, would replace Beyfortus
- Additional covariables might have improved estimation of Beyfortus effectiveness; however, data on these covariates were incomplete for most of the population
- Access to healthcare may have been limited in extreme regions of Chile and to undocumented migrants
Population health impact of Beyfortus on RSV hospitalization in Chile10

There were no pronounced safety events associated with the use of Beyfortus.10
RSV-LRTI hospitalization after Beyfortus implementation10

AE, adverse event; CI, confidence interval; ICD-10, International Classification of Diseases, Tenth Revision; LRTI, lower respiratory tract infection; RSV, respiratory syncytial virus; SD, standard deviation.
*Analysis of records from the National Hospital Discharge System, developed by the Department of Health Statistics and Information (DEIS) of the Ministry of Health. Records cover all hospital admissions in public (156 hospitals) and private (78 hospitals) institutions and document primary diagnosis using the ICD-10 classification standard and bed use during the hospitalization period.19
†Cumulative immunization coverage at the end of the 2024 RSV season, on epidemiologic Week 40.10
‡RSV hospitalization was defined as hospitalization for RSV-related LRTI.10
§Infants were considered to be immunized starting 7 days after receipt of Beyfortus to account for the possibility that infants were already infected with the virus at the time of immunization. Thus, eligible infants with RSV-related hospitalization in the first 7 days after immunization were considered nonimmunized.10
‖At the end of the RSV season, 957 RSV hospitalizations occurred among 145,087 immunized infants, and 327 occurred among 9,086 nonimmunized infants.10
¶The 2020 and 2021 seasons were not considered due to anomalies in RSV epidemiology caused by the COVID-19 pandemic.10
#Relative reduction of cases was calculated as 100 times the averted number of cases divided by the expected number of cases, with 30.05 averted cases per 1,000 infants.10
EPI-PHARE
Real-world effectiveness of Beyfortus vs maternal vaccination with RSVpreF in France.
Comparative analysis between Beyfortus and the RSVpreF vaccine11
Infants born between September 1 and December 31, 2024, in mainland France, who were immunized either via Beyfortus or maternal vaccination (RSVpreF) and were discharged from the hospital on or after October 1, 2024. Follow-up ended at the time of RSV hospitalization, unrelated death, or on February 28, 2025.11*
- For the 2024-2025 RSV season, daily RSV hospitalizations occurred from October 2024 to February 2025 and peaked from mid-November 2024 to early January 2025†
- In matched analysis: N=42,560; n=21,280 in each group
- In France, Beyfortus was recommended during the first RSV season for all infants born on or after January 1, 2024†
- Maternal vaccination with RSVpreF was recommended at 32 to 36 weeks’ gestation from September 1, 2024, to January 31, 2025‡
- Infants were matched 1:1 based on discharge day, sex, gestational age, and region of residence. Weighted conditional Cox proportional hazards models were fitted to account for the matched design and estimate hazard ratios (HRs) with 95% CIs§‖
Key assessment: Hospitalization for RSV-associated LRTI.11
Prevention of RSV hospitalization during the 2024-2025 season11
Primary outcome: RSV hospitalization11

The adjusted hazard ratio (aHR) was derived using an inverse probability of treatment weighting method that was applied to the matched dataset to further balance the residual covariates.11
The difference in hospitalization risk varied over time. Beyfortus showed11:
- Higher risk from Day 0 to Day 7 (aHR: 2.94; 95% CI: 1.19, 7.69)
- No significant difference from Day 8 to Day 30 (aHR: 0.79; 95% CI: 0.60, 1.05)
- Lower risk from Day 31 to Day 60 (aHR: 0.62; 95% CI: 0.45, 0.84)
- Lower risk after Day 60 (up to Day 148) (aHR: 0.51; 95% CI: 0.30, 0.86)
The findings in this report are subject to limitations11:
- As the RSVpreF vaccine became available in September and matching was based on birth date, infants were, by design born later in the RSV season, which may limit generalizability to those born earlier
- The study was conducted during the first season of maternal RSVpreF vaccination in France, when eligibility was limited to 32 to 36 weeks’ gestation, unlike the WHO’s recommendation for vaccination beginning at 28 weeks’ gestation. Findings reflect early national experience in France and require reevaluation in future studies and settings
- Follow-up was limited to one RSV season, so durability of protection could not be assessed
- Administrative data did not allow analysis by RSV subtypes
- The subgroup analyses were not stratified beyond 60 days of follow-up, limiting insights into longer-term differences between the 2 preventive strategies
- Potential unmeasured confounding factors (eg, parental health-seeking behavior, household smoking, or daycare attendance) could not be excluded
This study did not assess the safety of Beyfortus or RSVpreF.
CI, confidence interval; EPI-PHARE, French National Agency for Medicines and Health Products Safety and French National Health Insurance; ICD-10, International Classification of Diseases, Tenth Revision; IQR, interquartile range; LRTI, lower respiratory tract infection; MA, medically attended; RSV, respiratory syncytial virus; RSVpreF, respiratory syncytial virus prefusion F protein; wGA, weeks gestational age; WHO, World Health Organization.
*RSV hospitalization was defined as hospitalization for RSV-associated LRTI identified using ICD-10 RSV codes for acute bronchiolitis (J210), pneumonia (J121), and acute bronchitis (J205).11
†The immunization campaign began on September 15, 2024.11
‡The national campaign concluded on January 31, 2025.11
§For each day between October 1 and December 31, 2024, every infant born to a mother vaccinated with the RSVpreF vaccine was matched to an infant who received Beyfortus on the same maternity discharge day, using random sampling without replacement. This process achieved a match rate of 92%.11
‖Infants were excluded if they were discharged from the maternity ward before October 1, 2024.11
HARMONIE
HARMONIE assessed the reduction of RSV hospitalization with Beyfortus during the RSV season and through 180 days.12,13
Study design
Beyfortus was associated with a reduction in RSV hospitalization in healthy term and preterm infants (aged ≤12 months and born at ≥29 wGA) during the RSV season and through 180 days12,13*
The phase 3b HARMONIE study was a pragmatic, open-label, randomized, parallel, 2-arm trial that studied Beyfortus vs no intervention in healthy term and preterm infants ≤12 months (≥29 wGA) entering their first RSV season in France, Germany, or the United Kingdom. The RSV season ended on February 28, 2023, in each country.12†
Study results
Primary endpoint13
Overall incidence of RSV hospitalization caused by confirmed RSV infection, through the RSV season.13*†‡§

Secondary endpoint12
Overall incidence of RSV hospitalization through 180 days after randomization.12†‡§∥
50 mg IM dose if <5 kg weight, 100 mg IM dose if ≥5 kg weight12

In most of the continental US, the typical RSV season lasts through 5 months, the same length of time reported in the Beyfortus pivotal trials.1,20
Safety
Treatment-emergent adverse events (TEAEs) in safety analysis population: healthy infants aged ≤12 months, during 12 months following randomization12,21
Adverse events (AEs)¶ |
Beyfortus, %
|
No intervention, %
|
| Any TEAE | 80.0 | 79.4 |
| Immediate TEAE: ≤30 minutes post dosing/randomization | 0.7 | 0 |
| Any study treatment-related TEAE# | 2.5 | 0 |
| TEAE of special interest | 0.3 | <0.1 |
| Any serious TEAE | 6.5 | 5.5 |
| Any serious study treatment-related TEAE | <0.1 | 0 |
| Medically attended TEAE | 77.3 | 77.2 |
Most AEs in the 2 trial groups were grade 1 or 2 in severity.12
Limitations of study12
- The follow-up does not include a second RSV season, where most of the loss of efficacy would be expected to occur
- The possibility of bias exists because the study is unblinded; however, extensive efforts have been made to reduce the risk of bias, including the use of endpoints that are robust to the open-label nature of the study
- The HARMONIE study was conducted in the epidemiological setting typical for European countries, with a period of high RSV circulation followed by low circulation after February. The lower number of cases due to low viral circulation in the latter part of the follow-up makes it more difficult to definitively assess sustained protection
CI, confidence interval; IM, intramuscular; LRTI, lower respiratory tract infection; RRR, relative risk reduction; RSV, respiratory syncytial virus; wGA, weeks gestational age.
*RSV hospitalization was defined as hospitalization for RSV-associated LRTI with hospital admission and an RSV-positive test result.12
†Infants could be born before or during the RSV season, which began on September 11, 2022 (Week 37) in France; on October 9, 2022 (Week 41) in Germany; and on September 4, 2022 (Week 36) in the United Kingdom. The RSV season ended on February 28, 2023, in each country.12
‡Overall incidence of hospitalization for RSV-LRTI was defined as admission to the hospital on the basis of the treating physician’s decision and confirmation of RSV by means of a positive result of a test performed in accordance with routine practice, during the RSV season in France, Germany, and the United Kingdom.12
§Infants were randomized 1:1 to receive either a single IM injection of Beyfortus or standard of care (no intervention). For primary endpoint: N=8,058; Beyfortus n=4,037, no intervention n=4,021. For secondary endpoint: N=8,057; Beyfortus n=4,038, no intervention n=4,019. The characteristics of infants at randomization were similar in the 2 groups, and 85.2% of infants were ≥37 wGA at birth.12,13
||The 2-sided 95% Cl for the efficacy was calculated by an exact method assuming a binomial distribution of the number of RSV-LRTI hospitalizations in the Beyfortus group, conditional on the total number in both groups (described by Breslow and Day), and accounted for the follow-up time after randomization.12,13
¶Assessment of AE severity was based on the AE severity grading scales adapted from FDA Guidance for Industry: Toxicity Grading Scale for Healthy Adult and Adolescent Volunteers Enrolled in Preventive Vaccine Clinical Trials, September 2007.21
#The relationship between a TEAE and treatment was assessed as related or not related. A treatment-related TEAE was defined as a TEAE considered by the investigator as related to, or with an unknown or missing relationship to, treatment for participants who received Beyfortus on Day 1. An unknown or missing relationship between a TEAE and treatment for participants who received no intervention was considered not related (Medical Dictionary for Regulatory Activities Version 25.0).21
BEAR
Beyfortus effectiveness against medically attended respiratory syncytial virus (RSV) events in infants (BEAR) is an observational, retrospective cohort study that assessed the effectiveness of Beyfortus at Kaiser Permanente Northern California (KPNC) during the 2023-2024 RSV season.14
Study design
Beyfortus was associated with a reduction in MA RSV-LRTI and RSV hospitalization in healthy term US infants (aged <8 months and born at ≥37 wGA)14
This study included 31,900 healthy term infants aged <8 months (≥37 wGA), born on or after April 1, 2023, without a predefined high-risk condition during the 2023-2024 RSV season. Beyfortus was routinely administered beginning October 19, 2023, at KPNC.14*
- 15,647 infants received Beyfortus compared to 16,253 infants who were untreated14
Co-primary endpoints14:
- First episode of PCR-confirmed RSV-LRTI during the RSV season†
- Healthcare utilization, as measured by the total number of medical encounters related to each RSV-LRTI episode‡
Post hoc analysis14:
- RSV hospitalization§
Study results14
Estimated effectiveness against MA RSV-LRTI

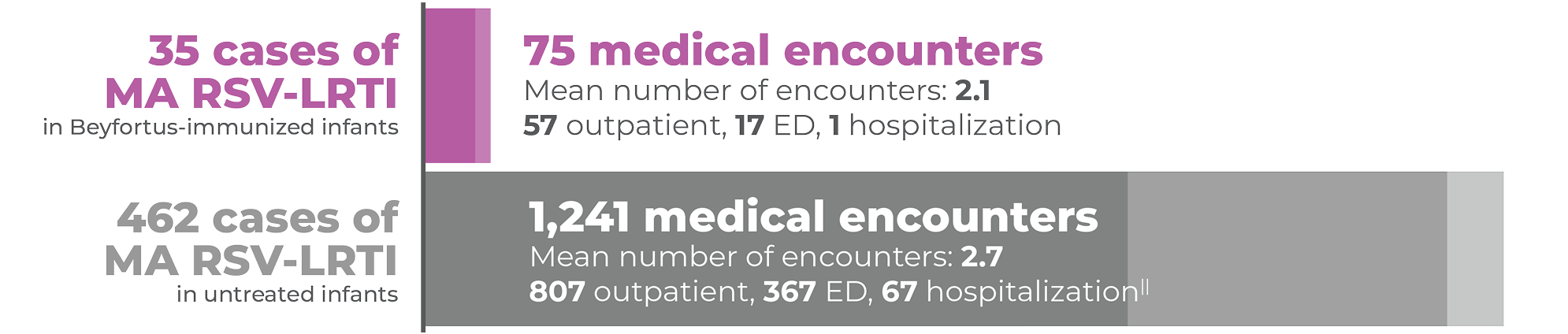
Infants immunized with Beyfortus had fewer medical encounters and were less likely to be hospitalized vs untreated infants14
Total RSV-LRTI medical encounters related to RSV-LRTI episodes14,22
Estimated effectiveness against RSV hospitalization14,22

Limitations of study14
- Investigators were unable to assess how soon RSV-LRTI protection occurs after receiving Beyfortus because few cases occurred within 7 days
- Although KPNC performs a large amount of PCR testing, investigators did not quantify what proportion of infants with respiratory symptoms were tested, so testing biases among RSV-positive infants were possible
- As an observational study, unmeasured confounders that increase one’s risk of RSV (eg, lower socioeconomic status, having siblings, and/or daycare attendance) could affect results
- The analysis population of healthy term infants may not be generalizable to infants at higher risk of RSV-LRTI
- While KPNC has a large and diverse population, the study population may not be representative of other health systems’ populations
CI, confidence interval; ED, emergency department; LRTI, lower respiratory tract infection; MA, medically attended; PCR, polymerase chain reaction; wGA, weeks gestational age.
*Eligible infants born on or after this date were offered the treatment before discharge, during urgent care visits, or at outpatient well-child appointments. Eligible infants born prior to this date were contacted by KPNC as part of routine care for catch-up dosing in outpatient clinics.14
†An episode is defined as having at least 1 LRTI-associated encounter in any setting in the 7 days before and up to 10 days after a positive RSV PCR test.14
‡Each medical encounter was categorized as outpatient, emergency department, inpatient, or intensive care unit.14
§Episodes that included at least 1 hospitalization were considered a hospitalized RSV-LRTI.14
‖There were 2 untreated infants who had 2 hospitalizations each during their RSV-LRTI episodes, with a total of 67 hospitalizations across all 65 RSV-LRTI episodes.22
CDC real-world data
The analysis was a population-based, prospective, active surveillance study that assessed the effectiveness of Beyfortus within the New Vaccine Surveillance Network (NVSN) during the 2023-2024 RSV season.15
Study design
Beyfortus was associated with preventing MA RSV ARI and RSV hospitalization in US infants (aged <8 months)15*
This study included infants <8 months as of October 1, 2023, or born after October 1, 2023, who had medically attended acute respiratory illness (ARI) between October 2023 and March 2024, who had verified Beyfortus status and medical records to assess underlying medical conditions, and were within the NVSN, which includes 7 sites.15,17†
- N=1,616 medically attended ARI (case patients receiving positive RSV test result, n=765; control patients receiving negative RSV test result, n=851)15‡
- Infants were considered Beyfortus recipients if they received Beyfortus ≥7 days before symptom onset17§
Study results15,17
Estimated effectiveness against MA RSV ARI||

Estimated effectiveness against RSV hospitalization15¶#

Among RSV isolates, there were no variants in the Beyfortus binding site on the F protein that would alter susceptibility of RSV to Beyfortus15
Limitations of study15
- NVSN sites may not be nationally representative
- Timing of Beyfortus availability resulted in a relatively short interval from administration to respiratory illness onset
- Beyfortus effectiveness over the course of a full RSV season is expected to be somewhat lower than this estimate because of antibody decay
CDC, Centers for Disease Control and Prevention; CI, confidence interval; ED, emergency department; IQR, interquartile range; MA, medically attended; RSV, respiratory syncytial virus.
*Medically attended RSV was defined as any medically attended RSV-associated ARI, and hospitalization was defined as RSV-associated hospitalization for ARI.17
†ARI is defined as one or more of the following signs or symptoms present for <14 days before enrollment encounter: apnea, cough, earache, fever, myalgia, nasal congestion, runny nose, sore throat, vomiting after coughing, shortness of breath (rapid or shallow breathing), wheezing, or apparent life-threatening event or brief resolved unexplained event.17
‡Ten out of 765 case patients who received Beyfortus were RSV positive compared with 126 out of 851 control patients who were negative for RSV.15,17
§Receipt of Beyfortus was ascertained through parent/guardian interviews, medical record abstraction, outpatient records, and state immunization information systems.15
‖Based on the median time from receipt of Beyfortus to symptom onset of 44 days (IQR=21-73 days).15,17
¶Based on the median time from receipt of Beyfortus to symptom onset of 41 days (IQR=18-68 days).17
#Of the 875 hospitalized patients, 531 (61%) were case patients with a positive RSV result and 344 (39%) were control patients with a negative RSV result. Six out of 531 case patients who received Beyfortus were RSV positive compared with 67 out of 344 control patients who were negative for RSV.15,17
Real-world evidence summaries for download
BEAR, Beyfortus Effectiveness Against Medically Attended RSV Events in Infants; CDC, Centers for Disease Control and Prevention; EPI-PHARE, French National Agency for Medicines and Health Products Safety and French National Health Insurance; RSVpreF, respiratory syncytial virus prefusion F protein.


Important Safety Information
References: 1. Beyfortus (nirsevimab-alip). Prescribing Information. Sanofi. 2. Data on File. Sanofi. 3. US Food and Drug Administration. Biologics license application 761328. June 8, 2023. Accessed May 28, 2026. https://www.fda.gov/media/169226/download 4. Muller WJ, Madhi SA, Nuñez BS, et al; MELODY Study Group. Nirsevimab for prevention of RSV in term and late-preterm infants. N Engl J Med. 2023;388(16)(suppl):1533-1534. 5. Muller WJ, Madhi SA, Nuñez BS, et al; MELODY Study Group. Nirsevimab for prevention of RSV in term and late-preterm infants. N Engl J Med. 2023;388(16):1533-1534. 6. Griffin MP, Yuan Y, Takas T, et al. Single-dose nirsevimab for prevention of RSV in preterm infants. N Engl J Med. 2020;383(5):415-425. 7. US Food and Drug Administration. Advisory Committee Briefing Document: nirsevimab. May 17, 2023. Accessed May 28, 2026. https://www.fda.gov/files/advisory committees/published/20230608-AMDAC-Backgrounder-AZ.pdf 8. Ares-Gómez S, Mallah N, Santiago-Pérez MI, et al; NIRSE-GAL study group. Effectiveness and impact of universal prophylaxis with nirsevimab in infants against hospitalisation for respiratory syncytial virus in Galicia, Spain: initial results of a population-based longitudinal study. Lancet Infect Dis. 2024;24(8):817-828. 9. Mallah N, Pardo-Seco J, Pérez-Martínez O, et al; NIRSE-GAL Study Group. Full 2023-24 season results of universal prophylaxis with nirsevimab in Galicia, Spain: the NIRSE-GAL study. Lancet Infect Dis. 2025;25(2):e62-e63. 10. Torres JP, Sauré D, Goic M, et al. Effectiveness and impact of nirsevimab in Chile during the first season of a national immunisation strategy against RSV (NIRSE-CL): a retrospective observational study. Lancet Infect Dis. 2025;25(11):1189-1198. 11. Jabagi MJ, Bertrand M, Gabet A, et al. Nirsevimab vs RSVpreF vaccine for respiratory syncytial virus-related hospitalization in newborns. JAMA. 2026;335(9):787-798. 12. Munro APS, Drysdale SB, Cathie K, et al; HARMONIE Study Group. 180-day efficacy of nirsevimab against hospitalisation for respiratory syncytial virus lower respiratory tract infections in infants (HARMONIE): a randomised, controlled, phase 3b trial. Lancet Child Adolesc Health. 2025;9(6):404-412. 13. Drysdale SB, Cathie K, Flamein F, et al; HARMONIE Study Group. Nirsevimab for prevention of hospitalizations due to RSV in infants. N Engl J Med. 2023;389(26):2425-2435. 14. Hsiao A, Hansen J, Fireman B, et al. Effectiveness of nirsevimab against RSV and RSV-related events in infants. Pediatrics. 2025;156(2):e2024069510. 15. Moline HL, Toepfer AP, Tannis A, et al; New Vaccine Surveillance Network Collaborators. Respiratory syncytial virus disease burden and nirsevimab effectiveness in young children from 2023-2024. JAMA Pediatr. 2025;179(2):179-187. 16. Mallah N, Pardo-Seco J, Pérez-Martínez O, et al; NIRSE-GAL Study Group. Full 2023-24 season results of universal prophylaxis with nirsevimab in Galicia, Spain: the NIRSE-GAL study. Lancet Infect Dis. 2025;25(2)(suppl):e62-e63. 17. Moline HL, Toepfer AP, Tannis A, et al; New Vaccine Surveillance Network Collaborators. Respiratory syncytial virus disease burden and nirsevimab effectiveness in young children from 2023-2024. JAMA Pediatr. 2025;179(2)(suppl):179-187. 18. Torres JP, Sauré D, Goic M, et al. Effectiveness and impact of nirsevimab in Chile during the first season of a national immunisation strategy against RSV (NIRSE-CL): a retrospective observational study. Lancet Infect Dis. 2025;25(11)(suppl):1189-1198. 19. NirseCL: monitoring the impact of nirsevimab in the winter campaign in 2024 in Chile—fifth report. Ministry of Health of Chile. January 17, 2025. 20. Obando-Pacheco P, Justicia-Grande AJ, Rivero-Calle I, et al. Respiratory syncytial virus seasonality: a global overview. J Infect Dis. 2018;217(9):1356-1364. 21. Munro APS, Drysdale SB, Cathie K, et al; HARMONIE Study Group. 180-day efficacy of nirsevimab against hospitalisation for respiratory syncytial virus lower respiratory tract infections in infants (HARMONIE): a randomised, controlled, phase 3b trial. Lancet Child Adolesc Health. 2025;9(6)(suppl):404-412. 22. Hsiao A, Hansen J, Fireman B, et al. Effectiveness of nirsevimab against RSV and RSV-related events in infants. Pediatrics. 2025;156(2)(suppl):e2024069510.
