- Article
- Source: Campus Sanofi
- 26 Mar 2026
GOLD 2026 Report: Key Updates for COPD Management
.2026-03-26-07-30-23.png)
Key Updates in the GOLD 2026 Report
- Burden of COPD: The section on the Burden of COPD has been updated with the latest epidemiological statistics and references.
- Screening and Case-Finding: The chapter on Screening and Case-Finding has been updated, and two new figures have been added (Figures 2.8 and 2.9).
- Vaccination Recommendations: Recommendations for people with COPD have been updated with the latest information on RSV and influenza vaccination.
- GOLD A, B, and E Categories: The criteria defining GOLD A, B, and E categories have been adjusted due to emerging evidence from observational studies. This evidence indicates that even one moderate or severe exacerbation prior to initiating maintenance pharmacological therapy increases the risk of subsequent events (Figures 3.7, 3.8, and 3.9). The threshold of one moderate exacerbation should now be used to consider treatment escalation, with the aim of achieving a low disease activity state characterized by no exacerbations.
- Disease Activity: A new section on Disease Activity has been included in the report.
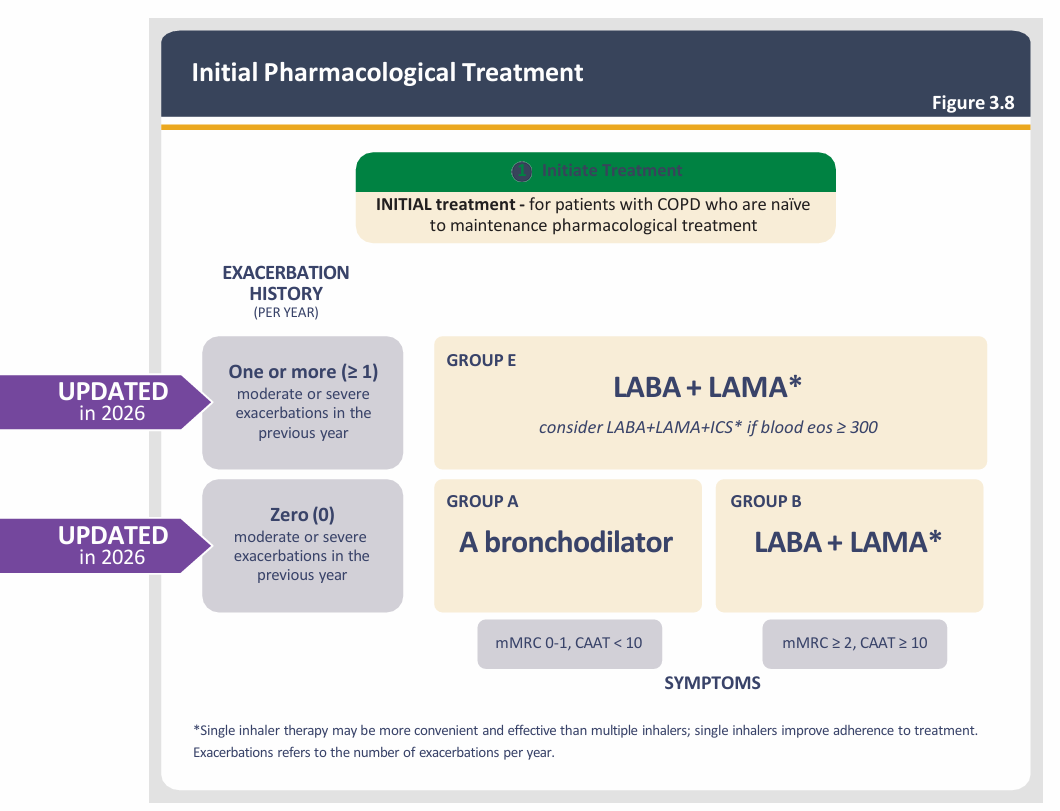
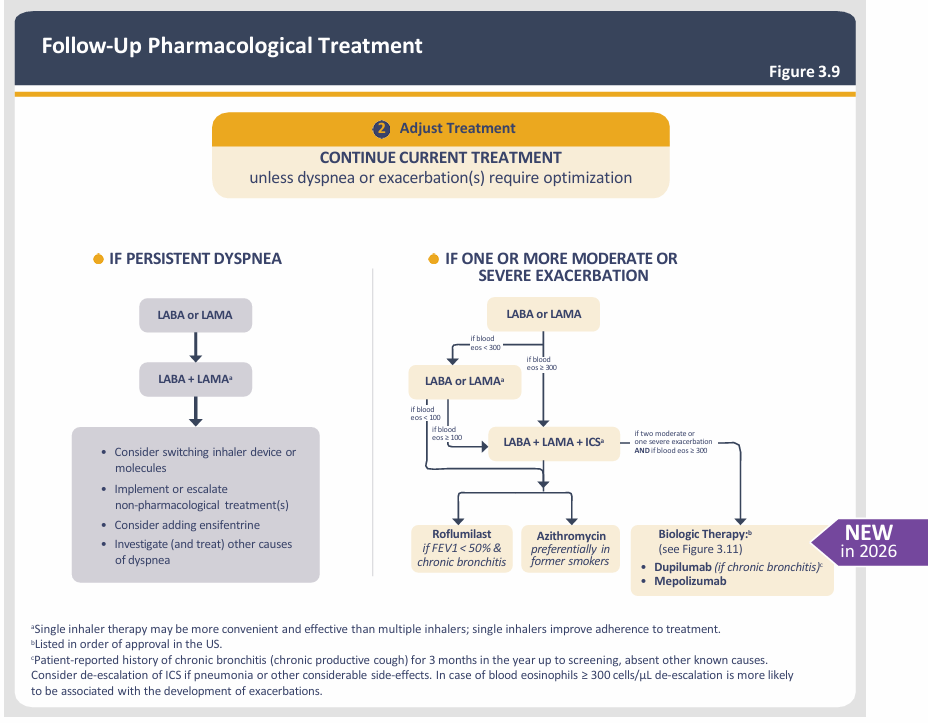
- Management Cycle and Treatment Algorithms: In Chapter 3, these have been further clarified to emphasize the distinction between INITIAL pharmacological treatment (for treatment-naïve COPD patients) and FOLLOW-UP pharmacological treatment (for patients on existing pharmacological treatment regimens), as shown in updated Figures 3.7, 3.8, and 3.9.
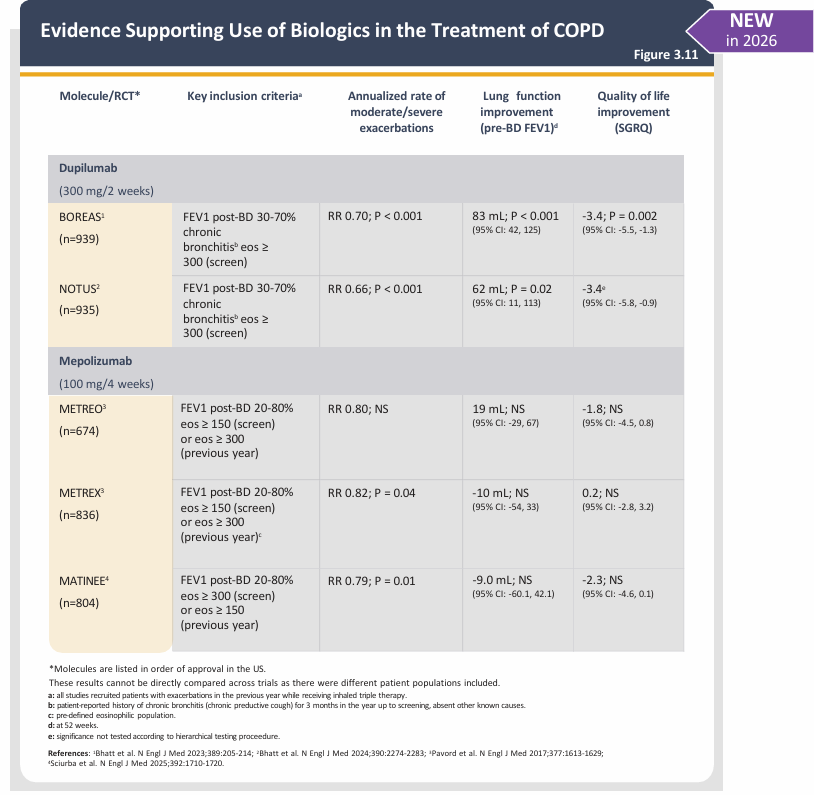
- Biologic Therapy: A new Figure 3.11 has been added to outline the evidence for the use of Biologic Therapy in COPD.
- Exacerbations of COPD: Chapter 4 has been completely revised, and new figures have been introduced.
- Multimorbidity in COPD: Chapter 5 has been completely revised, and new figures have been introduced.
- Artificial Intelligence & Emerging Technologies: A new Chapter 6 – Artificial Intelligence & Emerging Technologies in COPD – has been added.
- Report Restructuring: The GOLD Report has been restructured, with a significant amount of text and figures moved to Appendices 1–4 to improve flow, clarity, and reduce repetition.
- Abbreviations: A table of abbreviations has been included, and abbreviations are used throughout the report to improve readability.
- References: References have been checked and updated throughout the document.

What is Disease Activity in COPD?
Definition:
In chronic inflammatory diseases like COPD, disease activity refers to biological pathways that cause pathological outcomes and are potentially reversible with treatment.
Impact:
If left untreated or managed ineffectively, disease activity leads to disease progression, permanent organ damage, and dysfunction.

Key Concepts: Disease Stability vs Disease Control (NEW Definitions)

A low disease activity state with no exacerbations, no worsening of symptoms, and no accelerated loss of lung function.

A state of low disease activity, defined by no exacerbations and no worsening of symptoms, plus low impact on the patient, defined as symptoms below a threshold value.
How to Reduce Disease Activity
Pharmacological Treatment:
Anti-inflammatory drugs can reduce disease activity and prevent organ damage.
Non-Pharmacological Interventions:
Smoking cessation, pulmonary rehabilitation, and lung volume reduction can also reduce disease activity.
Assessment:
Monitoring biomarkers (e.g., blood eosinophil counts) and clinical features (exacerbations, worsening symptoms, lung function decline) is key to assessing disease activity and guiding treatment modulation.

UPDATED in 2026
- The criteria for GOLD A, B, and E categories have been updated, reflecting evidence that even one moderate or severe exacerbation increases future risk.
- Consequently, Group E has been modified to include individuals with one moderate exacerbation in the previous year.
- A single moderate exacerbation should now prompt consideration of treatment escalation.

UPDATED in 2026
- The algorithm for managing persistent exacerbations now includes mepolizumab following dupilumab as a biologic option.
- In patients on LABA + LAMA + ICS who have blood eosinophils ≥ 300 cells/µL and continue to experience exacerbations, consider adding dupilumab or mepolizumab.
- This follow-up pharmacological treatment algorithm can be applied to any patient who is already taking maintenance treatment(s), irrespective of the GOLD group allocated at treatment initiation.

NEW in 2026: Figure 3.11 has been added to outline the evidence and criteria for using biologic therapy in COPD.
MAT-BH-2500670