- Article
- Source: Campus Sanofi
- 12 May 2026
Management of ALLERGIC FUNGAL RHINOSINUSITIS (AFRS): A sever type 2 Inflammatory Disease
AFRS OVERVIEW
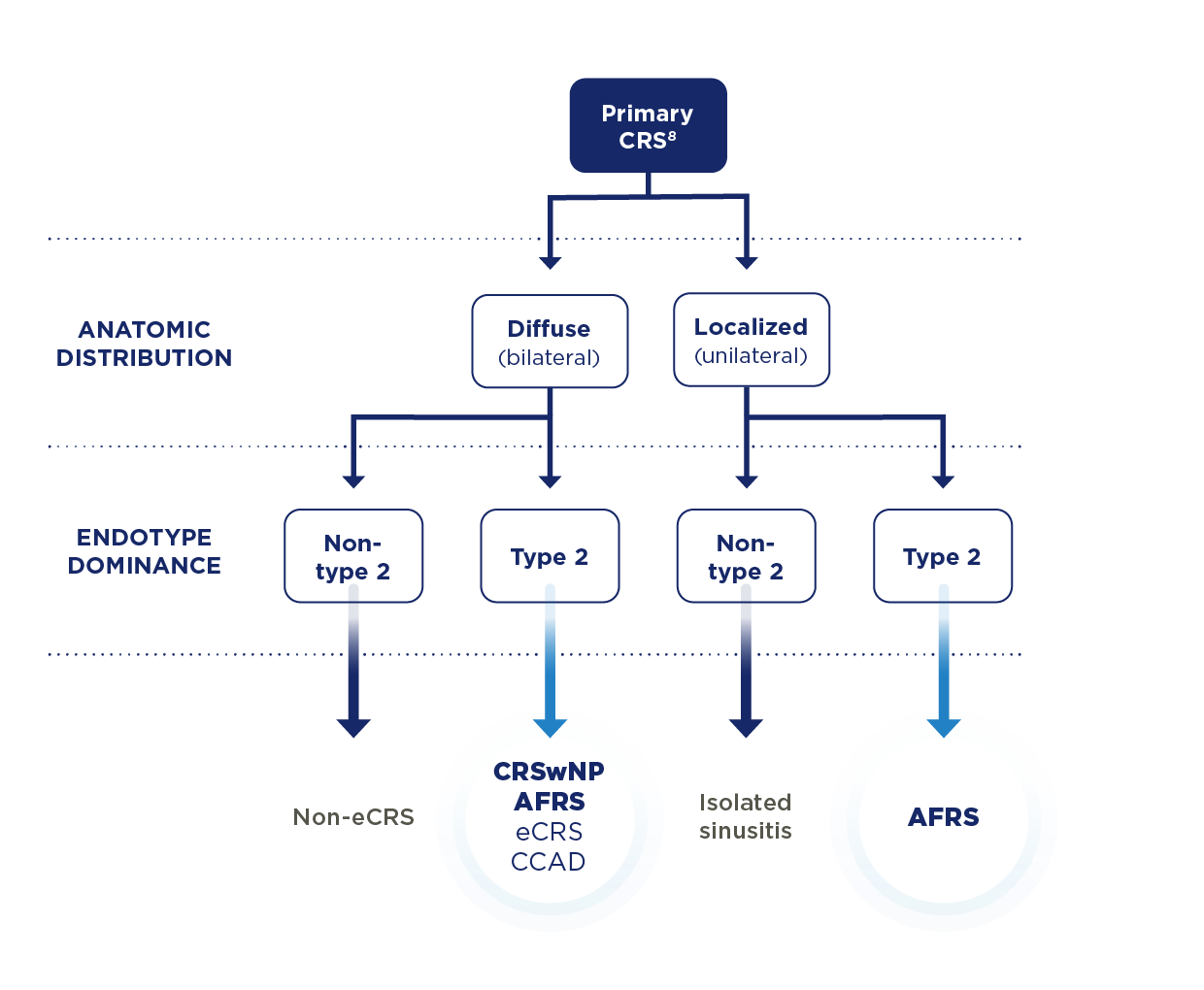
AFRS IS A DISTINCT SUBTYPE OF CHRONIC RHINOSINUSITIS (CRS) DRIVEN BY TYPE 2 INFLAMMATION4
AFRS affects ~12 million people worldwide, with highest prevalence observed in warm, humid regions1,5
AFRS is characterized by1,6:
- IgE-mediated hypersensitivity to fungal elements
- An accumulation of eosinophilic mucin within the sinuses
- Unilateral presentation of polyps is possible
Proactively identify AFRS to limit disease progression before structural damage occurs7
CCAD, central compartment allergy disease; CRSwNP, chronic rhinosinusitis with nasal polyps; eCRS, eosinophilic CRS.
DISTINCT FEATURES AND BURDEN
RECOGNIZE DISTINCT FEATURES OF AFRS BEFORE SEVERE STRUCTURAL DAMAGE OCCURS
While sharing features with CRS with nasal polyps, including polyp formation, type 2 inflammation, and eosinophilic mucin, AFRS exhibits defining clinical manifestations6




Uncontrolled AFRS can cause sinus remodeling and impact vision7,11
CURRENT TREATMENT LIMITATIONS
THE CURRENT STANDARD OF CARE OFFERS ONLY SHORT-TERM RESULTS IN AFRS3,12,13
Commonly used treatments leave patients with AFRS in a cycle of chronic inflammation and relapse3,12,13

SURGERY: THE MAINSTAY
OF AFRS MANAGEMENT
Surgery clears eosinophilic mucin, removes nasal polyps, and opens sinus cavities for nasal irrigations and INCS.
Challenges with surgery, such as incomplete debridement, have been linked to early recurrence and revision surgery3,9.
38% of patients experience recurrence within 1 year

SYSTEMIC STEROIDS:
AN ADJUVANT TO SURGERY
Pre-operative SCS reduce mucosal inflammation and decrease symptoms arising from mechanical obstruction. They also improve intraoperative visualization of sinonasal anatomy during FESS9.
Postoperative SCS may improve short-term outcomes and disease recurrence. However, they should be used with caution, since long-term use can cause a wide range of AEs across multiple organ systems, including1,9:
• Hyperglycemia • Infection • Poor wound healing
• Avascular necrosis • Increased ocular pressure
Antifungal agents and allergen immunotherapy are not recommended for the treatment of AFRS, according to the International Consensus Statement on Allergy and Rhinology14
Ongoing research aims to refine diagnostic criteria and optimize treatment options/selection and timing to enhance the treatment of AFRS6
AE, adverse event; FESS, functional endoscopic sinus surgery; INCS, intranasal corticosteroids; SCS, systemic corticosteroids.
SUMMARY
PATIENTS NEED MORE THAN THE CURRENT STANDARD OF CARE IN AFRS
Sinus surgery and systemic steroids have long-term limitations despite short-term benefits, leaving patients with AFRS at risk of symptom recurrence3,9
Address type 2 inflammation to limit structural damage in AFRS2
- Cameron BH, Luong AU. New developments in allergic fungal rhinosinusitis pathophysiology and treatment. Am J Rhinol Allergy. 2023;37(2):214-220. doi:10.1177/19458924231152983
- Roland LT, Damask C, Luong AU, et al. Allergic fungal rhinosinusitis diagnosis, management, associated conditions, pathophysiology, and future directions: summary of a multidisciplinary workshop. Int Forum Allergy Rhinol. 2025;15(6):626-641. doi:10.1002/alr.23582
- AlFadhel LK, Albarrak Y, AlFozan MS, Tatwani T. Postoperative recurrence in allergic fungal rhinosinusitis: a single center experience. Cureus. 2025;17(4):e81711. doi:10.7759/cureus.81711
- Cho SH, Hamilos DL, Han DH, Laidlaw TM. Phenotypes of chronic rhinosinusitis. J Allergy Clin Immunol Pract. 2020;8(5):1505-1511. doi:10.1016/j.jaip.2019.12.021
- Bongomin F, Gago S, Oladele RO, Denning DW. Global and multi-national prevalence of fungal diseases—estimate precision. J Fungi. 2017;3(4):57. doi:10.3390/jof3040057
- Chua AJ, Jafar A, Luong AU. Update on allergic fungal rhinosinusitis. Ann Allergy Asthma Immunol. 2023;131(3):300-306. doi:10.1016/j.anai.2023.02.018
- Al-Dousary S, Alarifi I, Bin Hazza’a A, Sumaily I. Paranasal sinus wall erosion and expansion in allergic fungal rhinosinusitis: an image scoring system. Cureus. 2019;11(12):e6395. doi:10.7759/cureus.6395
- Fokkens WJ, Lund VJ, Hopkins C, et al. European position paper on rhinosinusitis and nasal polyps 2020. Rhinology. 2020;58(suppl S29):1-464.
- Luong AU, Chua A, Alim BM, Olsson P, Javer A. Allergic fungal rhinosinusitis: the role and expectations of biologics. J Allergy Clin Immunol Pract. 2022;10(12):3156-3162. doi:10.1016/j.jaip.2022.08.021
- Tyler MA, Luong AU. Current understanding of allergic fungal rhinosinusitis. World J Otorhinolaryngol Head Neck Surg. 2018;4(3):179-185. doi:10.1016/j.wjorl.2018.08.003
- Alhussien A, Alghulikah A, Albaharna H, et al. Loss of vision outcome for allergic fungal rhinosinusitis: case report and literature review. Ther Adv Allergy Rhinol. 2023;14:1-7. doi:10.1177/27534030231176774
- Maspero J, Adir Y, Al-Ahmad M, et al. Type 2 inflammation in asthma and other airway diseases. ERJ Open Res. 2022;8(3):00576-2021. doi:10.1183/23120541.00576-2021
- Loftus CA, Soler ZM, Koochakzadeh S, et al. Revision surgery rates in chronic rhinosinusitis with nasal polyps: meta-analysis of risk factors. Int Forum Allergy Rhinol. 2020;10(2):199-207. doi:10.1002/alr.22487
- Orlandi RR, Kingdom TT, Smith TL, et al. International consensus statement on allergy and rhinology: rhinosinusitis 2021. Int Forum Allergy Rhinol. 2021;11(3):213-739. doi:10.1002/alr.22741
MAT-AE-2600412/v1/May2026