- Resource
- Source: Campus Sanofi
- 3 Jun 2025
Identify Your Patient
%20430x268.jpg)
Identify the very high-CV-risk patients in your practice
Determining the CV risk of your patients can be complex, especially when taking into consideration multiple risk factors.1
However, for patients who have had an ACS, determining CV risk is simple: all patients who have had an ACS event are classified as very high CV risk, even if they do not have any additional comorbidities.1 These patients may have been previously unidentified in your practice as very high CV risk and require urgent LDL-C management.1
Which of your patients are very high CV risk?
If we look at examples of the patients who may appear in your clinical practice, we can see a range of comorbidities and factors that contribute towards their CV risk:
Second MI
6 weeks ago
Age: 55 years
LDL-C: 112 mg/dL
Polyvascular disease
(CAD & PAD) Smoker

First MI
12 months ago
Age: 63 years
LDL-C: 102 mg/dL
Familial hypercholesterolaemia
Non-smoker
.2025-06-05-09-22-40.jpg)
First MI
6 months ago
Age: 63 years LDL-C: 130 mg/dL
No additional comorbidities or family history of heart disease
Non-smoker
.2025-06-05-09-22-40.jpg)
Hypothetical Patients
ESC/EAS guidelines definition of very high CV risk:1
- Documented ASCVD, such as previous ACS (MI or unstable angina)
-
Other documented ASCVD via imaging, CT scan or carotid ultrasound
-
DM with target organ damage, or ≥3 major risk factors, or early onset of Type 1 DM of long duration (>20 years)
-
Severe CKD (eGFR <30 mL/min/1.73 m2)
-
A calculated SCORE ≥10% for 10-year risk of fatal cardiovascular disease
-
FH with ASCVD or with another major risk factor
Any history of ACS means your patient is at very high CV risk, regardless of comorbidities1
Do your post-ACS patients require intensified LDL-C management?
As many as 40% of the patients in your practice may be classified by ESC/EAS guidelines as very high CV risk1,2*
Following their first ACS event, these patients are at immediate risk of a repeat CV event if their LDL-C is not rapidly controlled3
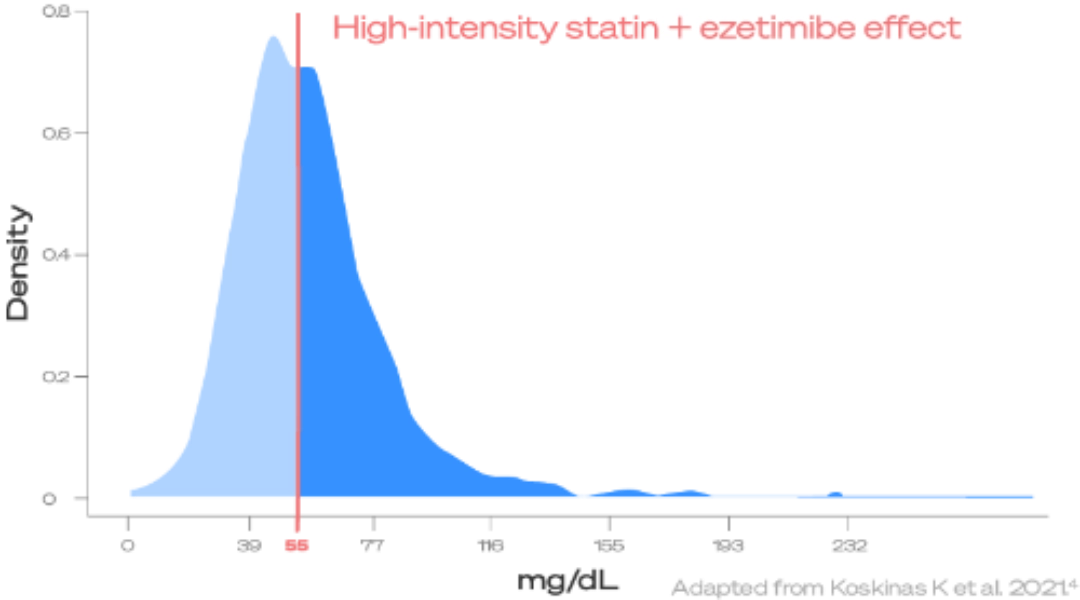
51% of very high-CV-risk patients would not reach ESC/EAS LDL-C goals4†
Currently there is still a gap in management of very high-CV-risk patients, and further work could be done to optimise post-ACS patient care.1,4.
*Using the British Heart Foundation Heart and Circulatory Disease Statistics 2021 document, data was taken from inpatient episodes by main diagnosis in NHS hospitals in the United Kingdom and calculated using ESC/EAS 2019 guidelines criteria for patients at very high CV risk: 304,745 (coronary heart disease) + 135,670 (stroke) + 24,961 (transient ischaemic attack and related syndromes) / 1,182,753 (all heart and circulatory diseases) x 100 = 39.35%.2 †At 1 year post index ACS event based on a modelled LDL-C level of <55 mg/ dL or greater on high-intensity statins and ezetimibe.4 The ELIPS study (NCT01075867) was a prospective, multicentre observational cohort study of consecutive ACS patients that aimed to assess the quality of care and adherence to recommended preventive treatments at four academic centres in Switzerland.4 The patient group contained 2,521 ACS patients enrolled between 1 January 2009 and 31 December 2017 who were alive one year after the index ACS event and had available data on LDL-C values and lipid lowering therapies.4
ACS = acute coronary syndrome; ASCVD = atherosclerotic cardiovascular disease; CKD = chronic kidney disease; CV = cardiovascular; DM = diabetes mellitus; EAS = European Atherosclerosis Society; eGFR = estimated glomerular filtration rate; FH = familial hypercholesterolaemia; LDL-C = low-density lipoprotein cholesterol; MI = myocardial infarcation; PAD = peripheral artery disease; SCORE = systematic coronary risk estimation;
-
Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41(1):111–188.
-
British Heart Foundation. Heart and Circulatory Disease Statistics 2021. Available at: https://www.bhf.org.uk/what-we-do/ our-research/heart-statistics/heart- statistics-publications/cardiovascular- disease-statistics-2021. Last accessed November 2021.
-
Jernberg T, Hasvold P, Henriksson M, et al. Cardiovascular risk in post-myocardial infarction patients: nationwide real-world data demonstrate the importance of a long-term perspective. Eur Heart J. 2015;36(19):1163–1170.
-
Koskinas KC, Gencer B, Nanchen D, et al. Eligibility for PCSK9 inhibitors based on the 2019 ESC/EAS and 2018 ACC/AHA guidelines. Eur J Prev Cardiol. 2021;28: 59–65.
MAT-BH-2200391/V2/JUN2024