
Beyfortus has been studied across multiple infant cohorts, including healthy, preterm, and at-risk infants, with consistent efficacy and safety data demonstrated in clinical trials. This page highlights key study designs, RSV hospitalization outcomes, and emerging real-world evidence.1-4
Summary of pivotal trials
Studied across a broad range of infant populations entering their first respiratory syncytial virus (RSV) season1
Healthy infants born term and late pretermTrial 04 (Phase 3 MELODY)1*
|
Healthy infants born pretermTrial 03 (Phase 2b)1 |
Infants at higher risk of severe RSV diseaseTrial 05 (Phase 2/3 MEDLEY)1,2,5‡
| |
Study population | Infants entering their first RSV season ≥35 weeks gestational age (wGA) | Infants entering their first RSV season ≥29 to <35 wGA |
2 cohorts:
|
Number of subjects |
N=1,490 (Beyfortus n=994, placebo n=496) |
N=1,453 (Beyfortus n=969, placebo n=484) |
N=925† (Beyfortus n=616, palivizumab n=309) |
Randomized, double-blind | 2:1 Beyfortus: placebo | 2:1 Beyfortus: palivizumab | |
Single Beyfortus intramuscular (IM) dose | 50 mg if <5 kg weight†
100 mg if ≥5 kg weight† | 50 mg for all weights† | 50 mg if <5 kg weight†
100 mg if ≥5 kg weight† |
Primary endpoint | Incidence of medically attended respiratory syncytial virus lower respiratory tract infection (MA RSV-LRTI) through 150 days post 1 dose | Safety and tolerability through 360 days post dose | |
Secondary endpoint | Incidence of MA RSV-LRTI requiring hospitalization through 150 days post 1 dose | Serum concentrations and pharmacokinetic (PK) parameters | |
*During Trial 04, the COVID-19 pandemic interrupted trial enrollment. The efficacy analysis is based on the Primary Cohort, which included participants enrolled prior to the pause due to COVID-19. Trial 04 continued monitoring the Primary Cohort and included an additional 1,522 subjects enrolled after the pause to comprise the full study cohort.6
†For neonates and infants in their first season, the recommended dosage is 50 mg for infants <5 kg or 100 mg for infants ≥5 kg administered via IM injection. For children up to 24 months of age who remain at increased risk for severe RSV disease in their second season, the recommended dosage is a single 200 mg dose, administered as 2 IM injections (2 x 100 mg).1
‡Included 128 preterm infants born at <29 wGA.1
Trial 04 efficacy
Trial 04 (Primary Cohort): healthy term and late preterm infants (≥35 wGA)1*†‡
Primary endpoint: Incidence of MA RSV-LRTI through 150 days post 1 dose.
Medically attended (MA) includes all healthcare provider visits, such as physician’s office, urgent care, emergency room, and hospitalizations.
Proven strong and consistent efficacy against RSV disease1

Signs of LRTI involvement included rhonchi, rales, crackles, or wheezing, and at least one sign of worsening clinical severity, including at least one of the following: increased respiratory rate, hypoxemia, acute hypoxic or ventilatory failure, new-onset apnea, nasal flaring, retractions, grunting, or dehydration due to respiratory distress.
CI, confidence interval; RRR, relative risk reduction.
*Primary Cohort: 1,490 healthy term and late preterm infants (≥35 wGA) in Trial 04.1
†The primary efficacy analysis for Trial 04 is based on infants from the Primary Cohort.1
‡Efficacy for MA RSV-LRTI is based on RRR against placebo, adjusted for age at randomization.1
Randomized, double-blind, placebo-controlled, multicenter Trial 041,3,7

Baseline characteristics: At randomization, 14% were ≥35 to <37 wGA; 86% were ≥37 wGA.1
The post hoc analysis of infants <5 kg receiving the 50 mg dose showed increased efficacy at this dosage strength compared to heavier infants in Trial 03.1
PCR, polymerase chain reaction.
*Signs of LRTI involvement included rhonchi, rales, crackles, or wheezing and at least one sign of worsening clinical severity, including at least one of the following: increased respiratory rate, hypoxemia, acute hypoxic or ventilatory failure, new onset apnea, nasal flaring, retractions, grunting, or dehydration due to respiratory distress.1
Study design with efficacy monitoring for 151 days and safety monitoring for 361+ days7
Trial 041
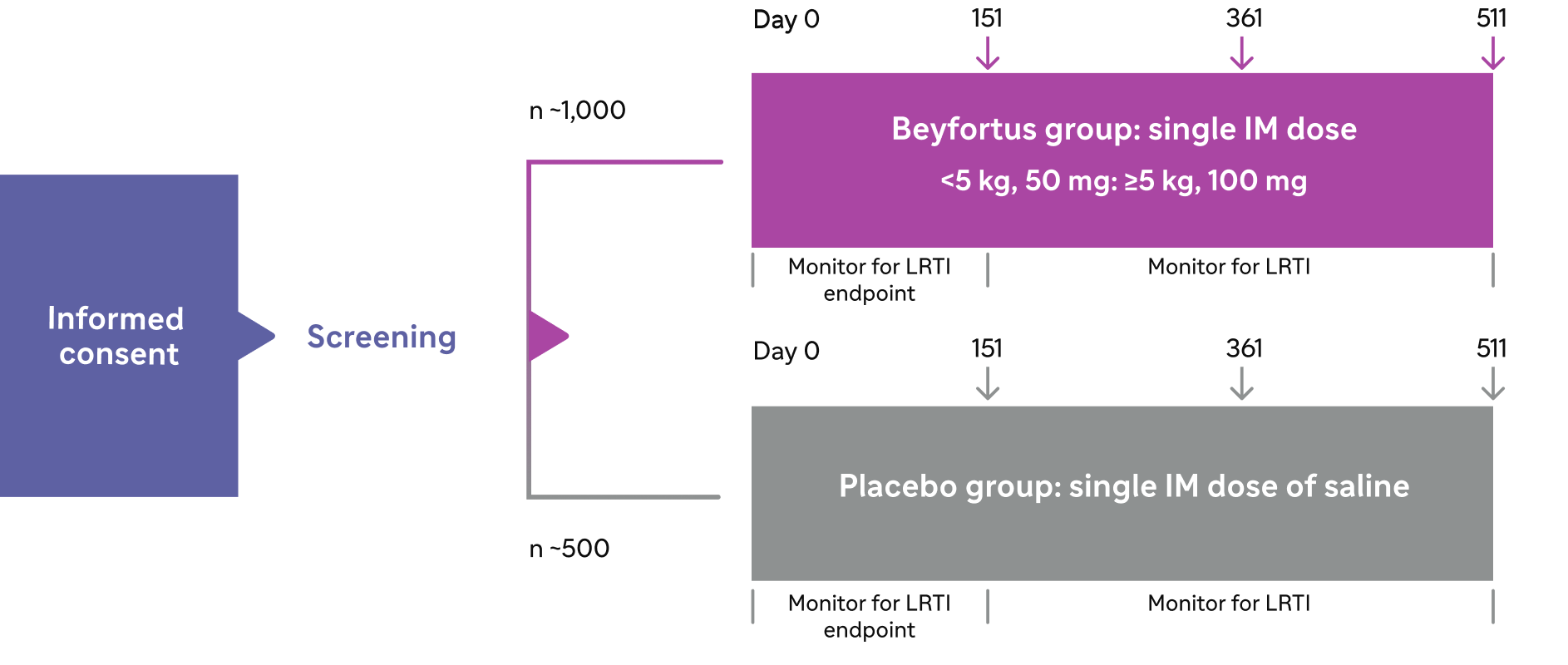
Post-dose follow-up visits: Day 151 was an efficacy evaluation; Days 361 and 511 were both safety evaluations entering the second season; final assessment via telephone call.
Beyfortus in RSV hospitalizations compared with placebo1,8
Trial 04: Incidence of RSV-LRTI requiring hospitalization through 150 days post 1 dose.
RSV hospitalization was defined as hospitalization for LRTI with a positive RSV test.1
Primary Cohort: Hospitalization endpoint.1,8
The Primary Cohort of Trial 04 included 1,490 infants randomized to receive Beyfortus (n=994) or placebo (n=496).

RRR based on a comparison of hospitalized infants8:
6 infants receiving Beyfortus (0.6%)
8 infants receiving placebo (1.6%)
Full study cohort: Exploratory post hoc analysis of the hospitalization endpoint.6,8,9
Trial 04 continued to enroll infants following the primary analysis; the full study cohort included 3,012 infants randomized to receive Beyfortus (n=2,009) or placebo (n=1,003) in this post hoc analysis.

RRR based on a comparison of hospitalized infants:
9 infants receiving Beyfortus (0.4%)
20 infants receiving placebo (2.0%)
The dose given was 50 mg for infants <5 kg or 100 mg for infants ≥5 kg via IM injection.1
- Most common adverse reactions with Beyfortus were rash (0.9%) and injection site reactions (0.3%)1
Trial 03 efficacy
Trial 03: healthy preterm infants (≥29 to <35 wGA)1*†
Primary endpoint: Incidence of MA RSV-LRTI through 150 days post 1 dose.
Medically attended (MA) includes all healthcare provider visits, such as physician’s office, urgent care, emergency room, and hospitalizations.
Proven strong and consistent efficacy against RSV disease1

Signs of LRTI involvement included rhonchi, rales, crackles, or wheezing, and at least one sign of worsening clinical severity, including at least one of the following: increased respiratory rate, hypoxemia, acute hypoxic or ventilatory failure, new-onset apnea, nasal flaring, retractions, grunting, or dehydration due to respiratory distress.
*1,453 preterm infants (≥29 to <35 wGA) in Trial 03.1
†Efficacy for MA RSV-LRTI is based on RRR against placebo, adjusted for age at randomization and hemisphere.1
Randomized, double-blind, placebo-controlled, multicenter Trial 031,4

Baseline characteristics: At randomization, 20% were ≥29 to <32 wGA; 80% were ≥32 to <35 wGA.1
The post hoc analysis of those <5 kg receiving the 50 mg dose showed increased efficacy at this dosage strength compared to heavier infants.1
*Signs of LRTI involvement included rhonchi, rales, crackles, or wheezing and at least one sign of worsening clinical severity, including at least one of the following: increased respiratory rate, hypoxemia, acute hypoxic or ventilatory failure, new onset apnea, nasal flaring, retractions, grunting, or dehydration due to respiratory distress.1
Study design with efficacy monitoring for 151 days and safety monitoring for 361 days10
Trial 034
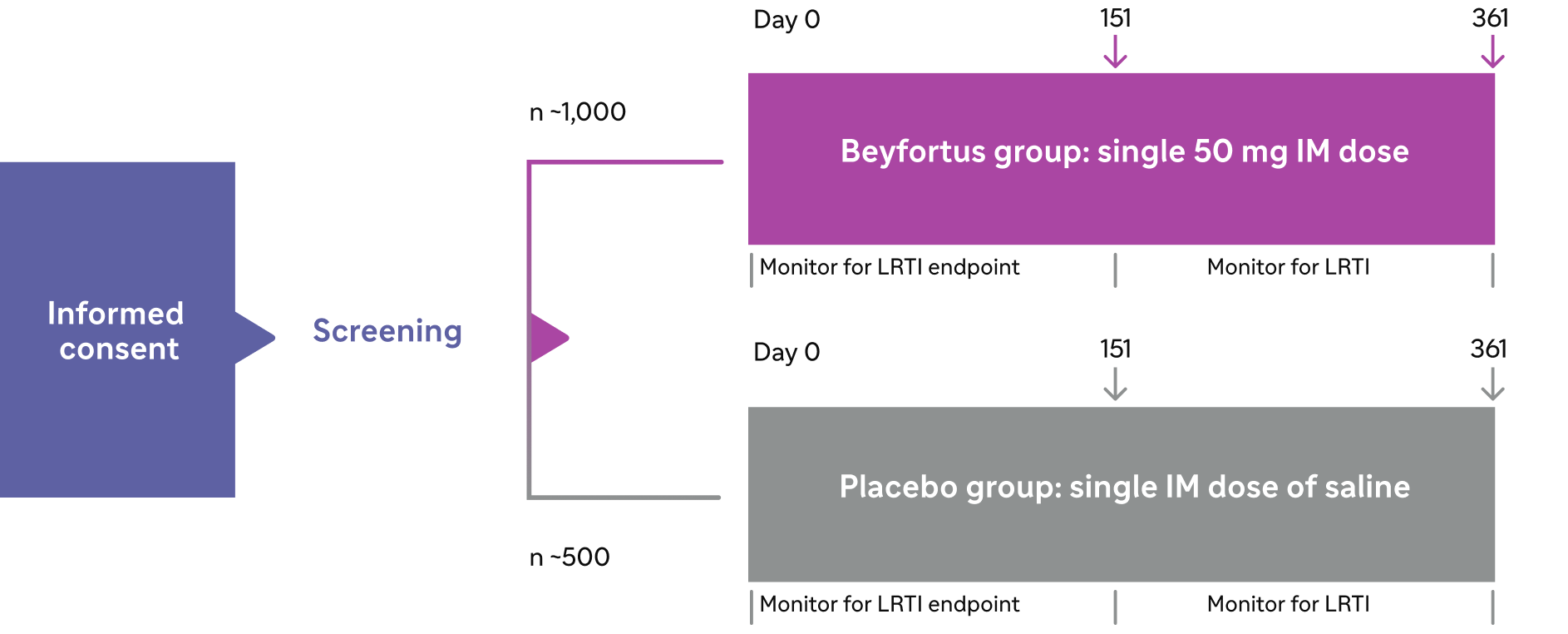
Post-dose follow-up visits: Day 151 was an efficacy evaluation; Day 361 was a safety evaluation entering the second season.
Trials 04 and 03 safety
Trial 04 and Trial 03 were pooled to evaluate the safety of Beyfortus (N=2,570) compared to placebo (N=1,284)1
Overall safety summary
1.2%
of infants receiving
Beyfortus reported ARs
97%
of ARs were mild to
moderate in severity
Most common adverse reactions reported at an incidence higher than placebo in the safety population*
Adverse reaction |
BeyfortusN=2,570 |
PlaceboN=1,284 |
| Rash†
(occurring within 14 days post dose) | 0.9% | 0.6% |
| Injection site reaction‡
(occurring within 7 days post dose) | 0.3% | 0.0% |
AR, adverse reaction.
*The Safety Population includes all infants who received the recommended dose of Beyfortus in Trials 04 and 03: Primary and Safety cohorts from Trial 04; infants who weighed <5 kg and who received the recommended dose of Beyfortus (single 50 mg IM dose) in Trial 03.1
†Rash was defined by the following grouped preferred terms: rash, rash macular, rash maculopapular, and rash papular.1
‡Injection site reaction was defined by the following grouped preferred terms: injection site reaction, injection site pain, injection site induration, injection site edema, and injection site swelling.1
Trial 05 safety and exploratory efficacy
Trial 05: analysis of Beyfortus vs palivizumab in infants at higher risk of severe RSV disease1
Safety
The safety of Beyfortus was evaluated in Trial 05, a Phase 2/3, randomized, double-blind, palivizumab-controlled, multicenter trial in infants and children at higher risk for severe RSV disease.
First RSV season1:
Infants who were eligible for palivizumab and born at <35 wGA or infants with CLD of prematurity and/or hemodynamically significant CHD.
Adverse reactions reported among Trial 05 infants who received Beyfortus in their first RSV season were similar to those in Trials 04 and 03.
Second RSV season1:
Children up to 24 months of age with CLD of prematurity and/or hemodynamically significant CHD.
The safety profile of Beyfortus in these children during their second RSV season was consistent with the safety profile of Beyfortus observed during their first RSV season.
First season study design: Randomized, double-blind, palivizumab-controlled, multicenter safety study1,5

Second season study design: Randomized, double-blind, palivizumab-controlled, multicenter safety study1,5

Forty children who received palivizumab in the first RSV season received Beyfortus in their second RSV season; and 42 children received palivizumab in both first and second RSV seasons.1
Baseline characteristics: At randomization, in the preterm cohort, 77 infants (13%) were <29 wGA and 499 (81%) were ≥29 to <35 wGA. In the CLD/CHD cohort, 70% had CLD; 34% had hemodynamically significant CHD; 123 infants (40%) were <29 wGA; 28% were ≥29 to <35 wGA; and 32% were ≥35 wGA.1
*Signs of LRTI involvement included rhonchi, rales, crackles, or wheezing and at least one sign of worsening clinical severity, including at least one of the following: increased respiratory rate, hypoxemia, acute hypoxic or ventilatory failure, new onset apnea, nasal flaring, retractions, grunting, or dehydration due to respiratory distress.1
In an exploratory study of preterm infants (<35 wGA) and those with CLD/CHD, there was a numerically lower incidence of MA RSV-LRTI with Beyfortus compared with palivizumab1,2*
|
Incidence of MA RSV-LRTI through 150 days
in the first RSV season

There were no cases of MA RSV-LRTI through 150 days in the second RSV season
*Trial 05 was a Phase 2/3, randomized, double-blind, palivizumab-controlled study evaluating the safety of Beyfortus in infants with CLD or CHD and preterm infants (<35 wGA) entering their first RSV season. Children up to 24 months with CLD or CHD could continue in Trial 05 and receive Beyfortus or palivizumab prior to their second RSV season.1
Discover real-world Beyfortus data
BEAR, Beyfortus Effectiveness Against Medically Attended RSV Events in Infants; CDC, Centers for Disease Control and Prevention; EPI-PHARE, French National Agency for Medicines and Health Products Safety and French National Health Insurance; RSVpreF, respiratory syncytial virus prefusion F protein.

Tested. Trusted. Demonstrated.


Important Safety Information
References: 1. Beyfortus (nirsevimab-alip). Prescribing Information. Sanofi. 2. Domachowske J, Madhi SA, Simões EAF, et al; MEDLEY Study Group. Safety of nirsevimab for RSV in infants with heart or lung disease or prematurity. N Engl J Med. 2022;386(9):892-894. 3. Hammitt LL, Dagan R, Yuan Y, et al; MELODY Study Group. Nirsevimab for prevention of RSV in healthy late-preterm and term infants. N Engl J Med. 2022;386(9):837-846. 4. Griffin MP, Yuan Y, Takas T, et al. Single-dose nirsevimab for prevention of RSV in preterm infants. N Engl J Med. 2020;383(5):415-425. 5. Domachowske J, Madhi SA, Simões EAF, et al; MEDLEY Study Group. Safety of nirsevimab for RSV in infants with heart or lung disease or prematurity. N Engl J Med. 2022;386(9)(suppl):892-894. 6. Muller WJ, Madhi SA, Nuñez BS, et al; MELODY Study Group. Nirsevimab for prevention of RSV in term and late-preterm infants. N Engl J Med. 2023;388(16)(suppl):1533-1534. 7. Hammitt LL, Dagan R, Yuan Y, et al; MELODY Study Group. Nirsevimab for prevention of RSV in healthy late-preterm and term infants. N Engl J Med. 2022;386(9)(suppl):837-846. 8. US Food and Drug Administration. Biologics license application 761328. June 8, 2023. Accessed June 1, 2026. https://www.fda.gov/media/169226/download 9. Muller WJ, Madhi SA, Nuñez BS, et al; MELODY Study Group. Nirsevimab for prevention of RSV in term and late-preterm infants. N Engl J Med. 2023;388(16):1533-1534. 10. Griffin MP, Yuan Y, Takas T, et al. Single-dose nirsevimab for prevention of RSV in preterm infants. N Engl J Med. 2020;383(5)(suppl):415-425. 11. Mallah N, Pardo-Seco J, Pérez-Martínez O, et al; NIRSE-GAL Study Group. Full 2023-24 season results of universal prophylaxis with nirsevimab in Galicia, Spain: the NIRSE-GAL study. Lancet Infect Dis. 2025;25(2):e62-e63. 12. Ares-Gómez S, Mallah N, Santiago-Pérez MI, et al; NIRSE-GAL study group. Effectiveness and impact of universal prophylaxis with nirsevimab in infants against hospitalisation for respiratory syncytial virus in Galicia, Spain: initial results of a population-based longitudinal study. Lancet Infect Dis. 2024;24(8):817-828. 13. Torres JP, Sauré D, Goic M, et al. Effectiveness and impact of nirsevimab in Chile during the first season of a national immunisation strategy against RSV (NIRSE-CL): a retrospective observational study. Lancet Infect Dis. 2025;25(11):1189-1198. 14. Jabagi MJ, Bertrand M, Gabet A, et al. Nirsevimab vs RSVpreF vaccine for respiratory syncytial virus-related hospitalization in newborns. JAMA. 2026;335(9):787-798. 15. Munro APS, Drysdale SB, Cathie K, et al; HARMONIE Study Group. 180-day efficacy of nirsevimab against hospitalisation for respiratory syncytial virus lower respiratory tract infections in infants (HARMONIE): a randomised, controlled, phase 3b trial. Lancet Child Adolesc Health. 2025;9(6):404-412. 16. Drysdale SB, Cathie K, Flamein F, et al; HARMONIE Study Group. Nirsevimab for prevention of hospitalizations due to RSV in infants. N Engl J Med. 2023;389(26):2425-2435. 17. Hsiao A, Hansen J, Fireman B, et al. Effectiveness of nirsevimab against RSV and RSV-related events in infants. Pediatrics. 2025;156(2):e2024069510. 18. Moline HL, Toepfer AP, Tannis A, et al; New Vaccine Surveillance Network Collaborators. Respiratory syncytial virus disease burden and nirsevimab effectiveness in young children from 2023-2024. JAMA Pediatr. 2025;179(2):179-187. 19. Moline HL, Toepfer AP, Tannis A, et al; New Vaccine Surveillance Network Collaborators. Respiratory syncytial virus disease burden and nirsevimab effectiveness in young children from 2023-2024. JAMA Pediatr. 2025;179(2)(suppl):179-187.
