.2025-02-19-14-39-47.svg)
Read about the meta-analysis comparing dronedarone vs. sotalol across four retrospective observational health claims databases

Relative Risk Reduction in CV Hospitalization Rate was Evaluated for MULTAQ® (dronedarone) Tablets and Sotalol1
A real-world meta-analysis was conducted in AAD-naive patients who initiated either MULTAQ or sotalol1
Relative risk reduction (RRR) in CV hospitalization rate was evaluated for MULTAQ and sotalol1

Study Limitations1
- This real-world evidence was collected outside of controlled clinical trials and has inherent limitations, including a lesser ability to control for confounding factors and selection bias. Therefore, causal inferences cannot be made, and no reliable conclusions can be drawn
- Treatment was not randomized in this study according to indication, which may lead to confounding
- Study excluded subtherapeutic doses of sotalol (<160 mg/d), which could eliminate patients with comorbidities such as renal impairment, a population which would potentially be more susceptible to adverse side effects and have higher overall risk
- For the CV hospitalization endpoint, the results are unable to distinguish between hospitalizations due to adverse safety events vs those resulting from treatment nonresponse
- Patients in the sotalol arm who initiated in the inpatient setting and discontinued during the hospitalization due to an adverse safety event are excluded
- Different follow-up times and reasons for censoring between arms in the Optum and MarketScan databases were observed
- Study was conducted as a meta-analysis combining 4 different databases with heterogeneity, which may lead to confounding
A meta-analysis of each database for CV hospitalization utilizing pharmacy claims and EHR data (N=46,550)1

I2=15.11%.
*Results above were aggregated using a fixed effects model. I2 statistic was used to assess heterogeneity.
Real-world evidence continues to expand our understanding of AF treatment patterns, including in patients managed after ablation procedures.
Dronedarone Versus Sotalol Following Catheter Ablation in Adults With Atrial Fibrillation, A Retrospective Analysis Study.
Study Design2
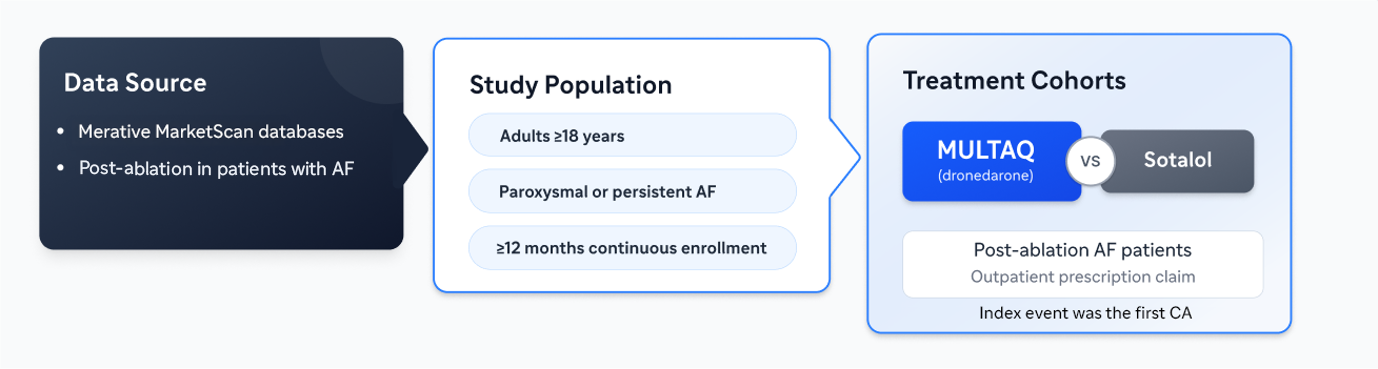
Study Population Included2:
- Adults (≥18 years) with a primary or secondary diagnosis of paroxysmal or persistent AF were eligible for inclusion with a first inpatient or outpatient claim for CA related to AF during the identification period
- ≥12 months' continuous health‑plan enrollment during the 12‑month baseline period
- An outpatient prescription claim for dronedarone or sotalol, on or after index
Key Exclusion Criteria2
- Patients with a diagnosis of ventricular arrhythmias, bradycardia, cardioverter defibrillator implantation, pacemaker implantation any time before the date of CA, and/or prescription claim(s) for another AAD (not dronedarone or sotalol) between index and the date of initiation of dronedarone or sotalol post-CA were excluded.
Study Limitations2
- Claims-based analysis; errors in data collection may lead to misclassification of certain diagnoses, events, or measures
- Findings may not generalize to US individuals without insurance, patients older or much younger than the data set (mean 61 years), and patients with AF in countries outside of the US
- Analysis could be impacted by survival bias, since post-CA patients who died before a dronedarone or sotalol prescription claim were excluded
- Inpatient prescription data were not available in the MarketScan databases. This is particularly relevant for the sotalol cohort, as sotalol is often initiated and dose-adjusted in the inpatient setting
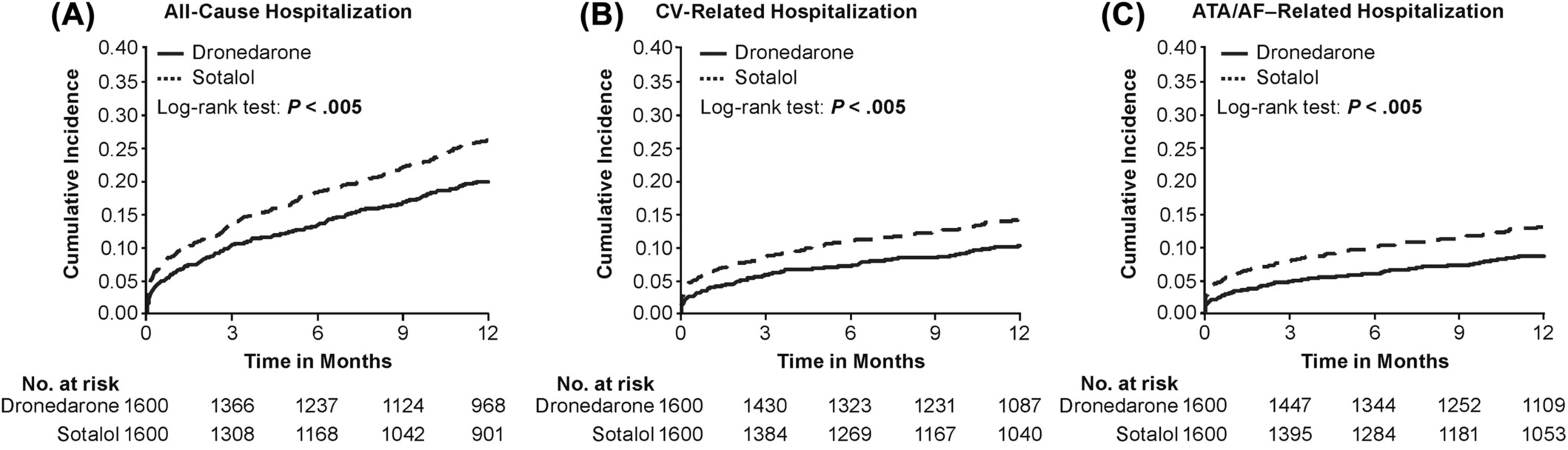
Study Results2
Cumulative incidence rates for (A) all-cause hospitalization, (B) CV-related hospitalization, (C) ATA/AF–related hospitalization, (all p<0.005) shown in figure below.
Prevalence rates (per 100-PY) for all-cause (24.0 vs. 27.4, p=0.003), CV-related (8.4 vs. 11.3, p<0.001),and ATA/AF-related hospitalizations (6.7 vs. 9.7, p<0.001) for dronedarone vs. sotalol, respectively.
For pacemaker implantation and repeat CA for patients within the dronedarone or sotalol cohorts after PSM over 12-months follow-up (not shown), Log-rank test P=.03 and P=.19 respectively. There is no head to head randomized controlled data comparing dronedarone to sotolol. See the full study
AAD, antiarrhythmic drug; AF, atrial fibrillation; ATA, atrial tachyarrhythmia; CA, catheter ablation; CDM, common data model; CI, confidence interval; CV, cardiovascular; EHR, electronic health records; FE, fixed effects; HR, hazard ratio; IBM, international business machines; NPR, national patient register; PSM, propensity score matching; PY, patient years; RRR, relative risk reduction; US, United States; VA, veterans affairs.
References:
1. Singh JP, Wieloch M, Reynolds SL, et al. Dronedarone vs Sotalol Among Patients With Atrial Fibrillation: A Meta-Analysis of Retrospective Observational Databases. JACC Clin Electrophysiol. 2025;11(7):1531-1542. 2. Zeitler EP, Stein D, Preblick R, et al. Health Care Resource Utilization With Dronedarone Versus Sotalol Following Catheter Ablation in Adults With Atrial Fibrillation. Clin Cardiol. 2025;48(1):e70064.

