Adult and Adolescent
With ELOCTATE individualized prophylaxis, adult and adolescent patients experienced a decrease in overall ABR over 5 years of clinical data1-4*
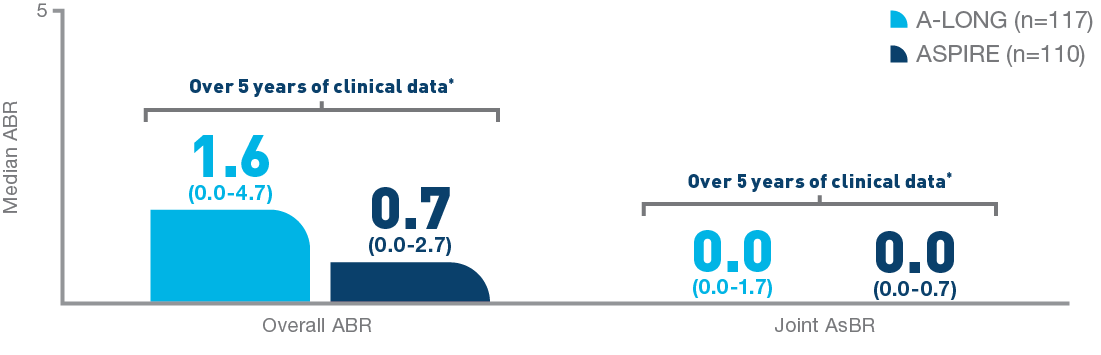
In the individualized prophylaxis arm, additional annualized bleed rates were1-3:
- AsBR: 0.0 (0.0-2.0) in A-LONG, 0.1 (0.0-1.1) in ASPIRE
- Traumatic ABR: 0.0 (0.0-1.8) in A-LONG, 0.2 (0.0-1.1) in ASPIRE
- Joint ABR: 0.0 (0.0-3.1) in A-LONG, 0.5 (0.0-1.7) in ASPIRE
In the A-LONG study, of 117 patients enrolled in the individualized prophylaxis arm, 112 were treated for ≥6 months. Dosing intervals were evaluated during the last 3 months of the study. Number of infusions may vary per individual. Individualized prophylaxis regimen: 25 IU/kg and 50 IU/kg of ELOCTATE on the first and fourth days of the week, respectively. Dose adjustments (25 to 65 IU/kg) and interval adjustments (every 3 to 5 days) were allowed based on a subject’s PK data and observed bleeding pattern.1
In the ASPIRE study, the individualized prophylaxis regimen was 25 to 65 IU/kg every 3 to 5 days or twice weekly (20 to 65 IU/kg on Day 1, 40 to 65 IU/kg on Day 4).2
Nearly 100% of target joints† were resolved with ELOCTATE prophylaxis5‡
- In 111 adult and adolescent patients taking ELOCTATE prophylaxis, 234 out of 235 target joints were resolved5
* The median cumulative treatment duration from the beginning of A-LONG to the end of ASPIRE was 4.5 years (range: 0.7 to 5.9 years).6
† A target joint is defined as a major joint with ≥3 bleeding episodes in a consecutive 6-month period. Target joint resolution is defined as ≤2 spontaneous bleeds in a 12-month period.5
‡Data based on a post-hoc analysis of the ASPIRE extension trial presented at EAHAD 2019. 54 adult and adolescent patients, and 56 pediatric patients, had no target joints at baseline when enrolled in A-LONG and Kids A-LONG, respectively.3,5,7
ABR=annualized bleed rate; AsBR=annualized spontaneous bleed rate; PK=pharmacokinetic.
ELOCTATE clinical trial experience demonstrated safety and efficacy in previously treated patients1

A-LONG Pivotal Trial1-3
- Multicenter, prospective, open-label, phase 3 study that evaluated the safety, efficacy, and PK of ELOCTATE for prophylaxis, treatment of acute bleeding, and perioperative hemostatic control
- Enrolled a total of 165 previously treated males aged 12 to 65 years with severe hemophilia A
- Included 113 patients with ≥1 target joint at baseline
- 6.0 prestudy median ABR among patients treated with prophylaxis
Kids A-LONG Pivotal Trial1,7
- Multicenter, open-label, phase 3 study that evaluated the safety and efficacy of ELOCTATE for prophylaxis, treatment of acute bleeding, and perioperative hemostatic control
- The primary endpoint was the development of inhibitors; key secondary endpoints included the PK profile of ELOCTATE, ABR, dose administered for treatment of a bleeding episode, and patients’ rating of response to ELOCTATE for the treatment of bleeding
- Enrolled a total of 71 previously treated males aged <12 years with severe hemophilia A; 69 patients (1–5 years of age, n=35; 6–11 years of age, n=34) were evaluable for safety and efficacy; 61 patients (88.4%) had >50 ELOCTATE EDs on study
- Included 13 patients with target joints
ASPIRE Extension Trial6
- Multicenter, open-label, nonrandomized evaluation of ELOCTATE in 150 previously treated males ≥12 years of age and 61 previously treated males <12 years of age with severe hemophilia A who completed the A-LONG or Kids A-LONG pivotal trials
- The primary endpoint was development of inhibitors (neutralizing antibodies). Key secondary endpoints included ABR, EDs, and subject’s assessment of response to treatment of a bleeding episode
- The median treatment duration from the beginning of A-LONG to the end of ASPIRE was 4.5 years (range: 0.7 to 5.9 years)
- The median treatment duration from the beginning of Kids A-LONG to the end of ASPIRE was 3.5 years (range: 0 to 4.4 years)
Across A-LONG and ASPIRE, 22 patients underwent 24 major surgeries. One surgery was not evaluable because the patient received a nonstudy drug.8
Additional ABR Cohorts
Median ABRs among adult and adolescent patients over 5 years of clinical data1,2,4,9
| A-LONG Individualized prophylaxis (n=117) | ASPIRE Individualized prophylaxis (n=110) | A-LONG On-demand (n=23) | ASPIRE On-demand (n=13) | |
| Overall ABR | 1.6 (0.0–4.7) | 0.74 (0.00–2.68) | 33.6 (21.1–48.7) | 19.10 (15.12–30.46) |
| Spontaneous ABR | 0.0 (0.0–2.0) | 0.10 (0.00–1.06) | 20.2 (12.2–36.8) | 14.61 (10.88–16.37) |
| Joint ABR | 0.0 (0.0–3.1) | 0.49 (0.00–1.70) | 22.8 (15.1–39.0) | 13.05 (7.35–26.97) |
Median ABRs among pediatric patients over 4 years of clinical data1,2,10
| Kids A-LONG (n=69) | ASPIRE (n=59) | ||
| <12 years | <6 years | 6 to <12 years | |
| Overall ABR | 2.0 (0.0–4.0) | 1.2 (0.6–2.4) | 1.6 (0.6–3.6) |
| Spontaneous ABR | 0.0 (0.0–0.0) | 0.6 (0.0–0.9) | 0.3 (0.0–0.9) |
| Joint ABR | 0.0 (0.0–2.0) | 0.6 (0.0–1.3) | 0.7 (0.0–1.7) |
Bleed control
Nearly all bleeds were controlled with ≤2 infusions of ELOCTATE6
.2025-02-20-13-22-04.svg)
Perioperative management
In 100% of assessed surgeries, hemostatic response with ELOCTATE was rated as “excellent” or “good”1||
- For 41 major surgeries in 29 patients from A-LONG or ASPIRE, hemostatic response was assessed and rated as excellent in 38 (93%) surgeries and good in 3 (7%) surgeries
- In 72 minor surgical procedures in 59 patients from all 3 studies, all (100%) had excellent response (61 of 72; 84.7%) or good response (11 of 72; 15.3%)
| Major surgeries from A-LONG and ASPIRE8 | |||
| Type of Surgery | Number of Procedures (Number of Patients) | Hemostatic Responseb | |
| Excellent | Good | ||
| Major surgery | 23a (22) | 19 | 3 |
| Arthrodesis | 1 (1) | 1 | – |
| Ankle fusion | 2 (2) | 2 | – |
| Appendectomy | 1 (1) | 1 | – |
| Arthroscopy | 2 (2) | 2 | – |
| Ventriculostomy | 1 (1) | 1 | – |
| Laparoscopic hernia surgery | 2 (2) | 1 | 1 |
| Discopathy repair | 1 (1) | 1 | – |
| Decompression of spine stenosis | 1 (1) | 1 | – |
| Arthroplastyc | 11 (10) | 9 | 1 |
| Knee arthroplasty converted to amputation | 1 (1) | – | 1 |
a Across A-LONG and ASPIRE, 22 patients underwent 24 major surgeries. One surgery was not evaluable because the patient received a nonstudy drug.
b Results based on a 4-point scale of excellent, good, fair, and poor/none. The median dose per infusion was 58.3 IU/kg (range, 45–102 IU/kg). The total dose on the day of surgery ranged from 50.8 to 126.6 IU/kg.
c One surgical rating was not available.
|| Major Surgeries: Hemostasis was assessed in 45 surgeries in 32 subjects from the A-LONG and ASPIRE studies. There were no major surgeries in the Kids A-LONG study. Of the 45 major surgeries, 36 surgeries (80.0%) required a single perioperative dose to maintain hemostasis. Of the 42 major surgeries treated with at least one dose, the median average dose per injection to maintain hemostasis during surgery was 59.1 IU/kg (range: 35–111). On the day of surgery, most subjects received a second injection. The total dose on the day of surgery ranged from 37.6–157.9 IU/kg. 1
Minor Surgeries: A hemostatic assessment of 72 minor surgical procedures in 59 subjects from all 3 studies was conducted. “Excellent” was defined as intraoperative and postoperative blood loss similar to (or less than) the nonhemophilic patient. No extra doses of ELOCTATE needed, and blood component transfusions required are similar to nonhemophilic patient. “Good” was defined as intraoperative and/or postoperative bleeding slightly increased over expectations for the nonhemophilic patient, but the difference was not clinically significant. Intraoperative blood loss no more than 250 mL greater than expected for a nonhemophilic patient, no extra doses of ELOCTATE needed, and blood component transfusions required are similar to nonhemophilic patient.1
INDICATION
References: 1. ELOCTATE [package insert]. Waltham, MA: Bioverativ Therapeutics Inc. 2. Nolan B, et al. Poster presented at: 60th American Society of Hematology Annual Meeting & Exposition; December 2018; San Diego, CA. 3. Mahlangu J et al. Blood. 2014;123(3):317-325. 4. Konkle B, et al. Poster presented at: 12th Annual Congress of the European Association for Haemophilia and Allied Disorders; February 2019; Prague, Czech Republic. 5. Oldenburg J, et al. Poster presented at: 12th Annual Congress of the European Association for Haemophilia and Allied Disorders; February 6-8, 2019; Prague, Czech Republic Poster P158. 6. Nolan B et al. Haemophilia. 2020;26(3):494-502. 7. Young G et al. J Thromb Haemost. 2015;13:1-11. 8. Mahlangu J et al. J Thromb Haemost. 2016;116(1):1-8. 9. Nolan B et al. Haemophilia. 2020;26(suppl.):494-502. 10. Konkle B et al. Res Pract Thromb Haemost. 2023;7(6):102180.
