- Artikel
- Bron: Campus Sanofi
- 12 jun 2026
Biomarkers in Asthma: Early Intervention with Precision Medicine
9/10 patients with severe asthma have underlying type 2 inflammation.2,* This disease progression may be prevented by early targeted treatment of the inflammation.3
The importance of early targeted intervention in T2 Asthma2
Early treatment of type 2 Asthma with biologics:

Prevents OCS-use and associated adverse events3

May prevent irreversible damage of lung tissue3

May increase the chance of remission3
Prevents OCS-use and associated adverse events3
May prevent irreversible damage of lung tissue3
May increase the chance of remission3
Listen to Prof. Alberto Papi about the importance of early intervention
Type 2 biomarkers as predictive tools for assessing Asthma Attack
Type 2 inflammation can be identified by two independent and complementary biomarkers:
|
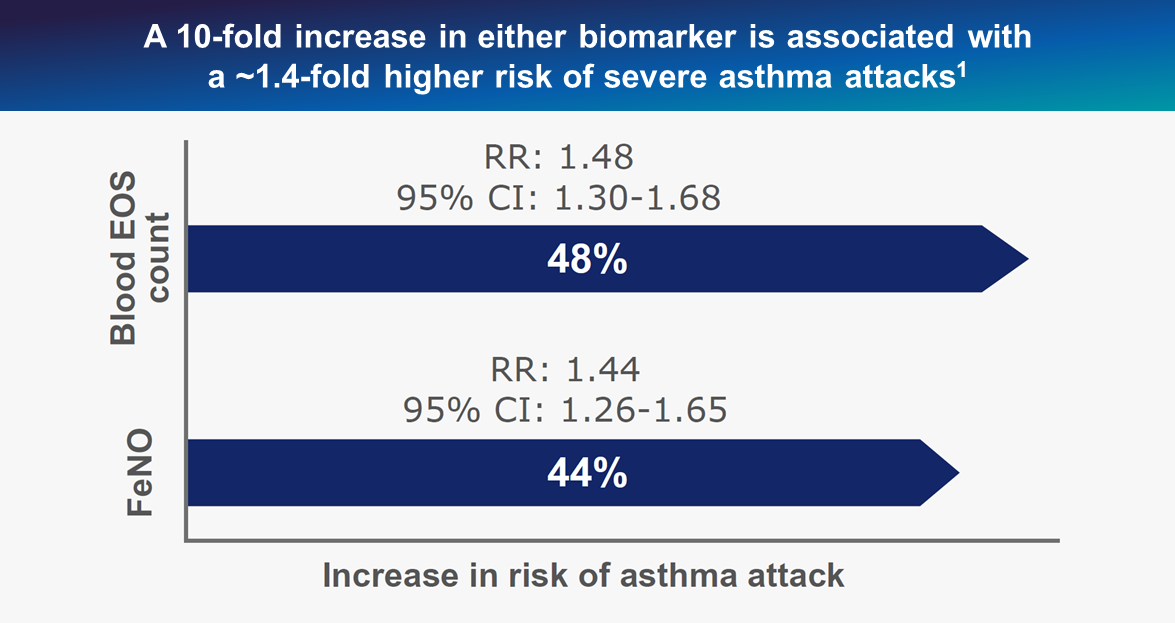
FeNO and blood eosinophils serve as more than diagnostic markers: they are predictive indicators of disease progression and treatment response.4,5
Patients at risk of exacerbations can already be identified at an early stage with these 2 biomarkers.1
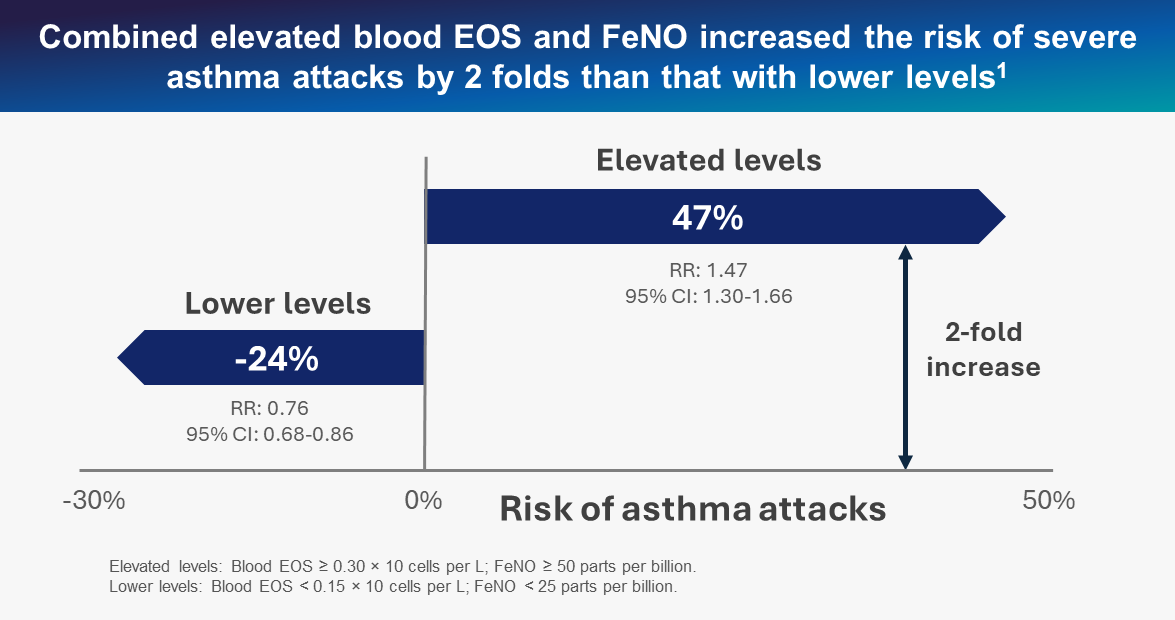
Did you know? |
Combined elevated EOS and FeNO levels even indicate a 2-fold risk-increase of severe asthma attacks compared to lower levels.1 |
Targeted Asthma treatment with biologics2
Where oral corticosteroids (OCS) primarily target symptoms, biologics specifically inhibit key cytokines involved in the inflammatory process (e.g. IL-4 and IL-13).6,7 Combined with biomarkers, this allows for a personalized treatment and monitoring approach.8,9 Importantly, biologics can not only reduce symptoms but may also modify the disease course.2
The benefits of biologics:
Reduce corticosteroid use and associated adverse events10

Reduced exacerbations and improved lung function10,11

Personalized treatment approach11

Lower emergency department visit and healthcare burden12
Reduce corticosteroid use and associated adverse events10
Reduced exacerbations and improved lung function10,11
Personalized treatment approach11
Lower emergency department visit and healthcare burden12
Learn more about key cytokines with Prof. Lipworth’s explanatory video
Although widely prescribed for asthma, OCS use is associated for some patients with poor disease control, a high risk of exacerbations, and higher morbidity and mortality.8,11 Even occasional short courses of OCS for acute exacerbations may cause significant short-term and cumulative long-term adverse effects, with a clear dose–response relationship.4
Did you know? |
93% of type 2 asthma patients using OCS experience at least one OCS-related side effect.13 |
Side effects with short-term use of OCS13 |
Side effects with long-term use of OCS13 | ||
Mental
|
Physical
|
Mental
|
Physical
|
The first OCS burst is the first sign to assess for type 2 asthma4,14-16
The GINA guideline recommends early initiation of biologic treatment in patients with asthma and the following type 2 inflammation characteristics:4

Blood eosinophil ≥150/μL and or sputum eosinophil level ≥2%4

FeNO ≥204

Clinically allergen-driven asthma4
Blood eosinophil ≥150/μL and or sputum eosinophil level ≥2%4
FeNO ≥204
Clinically allergen-driven asthma4
It is important to note that mOCS can suppress these biomarkers, making detection challenging. Therefore, biomarker testing should be repeated up to three times, ideally 1-2 weeks after OCS discontinuation or on the lowest possible OCS dose.4,5
The GINA guideline furthermore recommends:4
- Proactive phenotyping using biomarker assessment
- Early initiation of biologics before OCS dependency develops
- Systematic OCS tapering in patients receiving maintenance therapy
- Regular monitoring and treatment optimization
Key message |
Early assessment of the EOS and FeNO biomarkers and targeted treatment of type 2 inflammation with biologicals can improve the trajectory of asthma progression in your patients. |
*Up to 88% of adult patients may have T2 inflammation. T2 inflammation is defined as 1 of 3 phenotypes: eosinophilic asthma (blood eosinophils ≥150 cells/μL); atopic asthma allergen-specific IgE ≥0.35 IU/mL for any of 9 perennial allergens); Th2-high asthma (total serum IgE ≥100 IU/mL + blood eosinophils ≥140 cells/μL).1
-
Meulmeester FL, Mailhot-Larouche S, Celis-Preciado C, et al. Inflammatory and clinical risk factors for asthma attacks (ORACLE2): a patient-level meta-analysis of control groups of 22 randomised trials. Lancet Respir Med. Published online April 8, 2025. doi:10.1016/S2213-2600(25)00037-2.
-
Buhl R, Korn S, Menzies-Gow A, et al. ProspecJ AllergyClin Immunol Pract. 2020;8(8):2630-2639.e6. doi:10.1016/j.jaip.2020.03.038.
-
Tomasello A, Benfante A, Principe S, Scichilone N. Early Initiation of Biologic Therapies to Prevent Severe Asthma Progression. Medicina (Kaunas). 2025 Oct 6;61(10):1797. doi: 10.3390/medicina61101797. PMID: 41155784; PMCID: PMC12565776.
-
Global Strategy for Asthma Management and Prevention (2026 update) Available from: 2026 GINA Main Report - Global Initiative for Asthma - GINA (ginasthma.org). Accessed May 8, 2026.
-
Bourdin A, Brusselle G, Couillard S, et al. Phenotyping of Severe Asthma in the Era of Broad-Acting Anti-Asthma Biologics. J Allergy Clin Immunol Pract. 2024;12(4):809-823.
-
Howell I, Howell A, Pavord ID. Type 2 inflammation and biological therapies in asthma: Targeted medicine taking flight. J Exp Med. 2023;220(7):e20221212
-
Salter B, Lacy P, Mukherjee M. Biologics in asthma: A molecular perspective to precision medicine. Front. Pharmacol. 2022;12:793409.
-
Calzetta L, Aiello M, Frizzelli A, et al. Oral Corticosteroids Dependence and Biologic Drugs in Severe Asthma: Myths or Facts? A Systematic Review of Real-World Evidence. Int J Mol Sci. 2021;22(13):7132.
-
Phinyo P, Krikeerati T, Vichara-Anont I, et al. Efficacy and Safety of Biologics for Oral Corticosteroid-Dependent Asthma: A Systematic Review Network Meta-Analysis. J Allergy Clin and Immunol Pract. 2024;12(2):409.
-
Hansen S, Søndergaard MB, von Bülow A, et al. Clinical response and remission in patients with severe asthma treated with biologic therapies. CHEST. 2024; 165(2):253-266.
-
McGregor MC, Krings JG, Nair P, et al. Role of Biologics in Asthma. Am J Respir Crit Care Med. 2019;199(4):433–445.
-
Kavanagh JE, Hearn AP, Jackson DJ. A pragmatic guide to choosing biologic therapies in severe asthma. Breathe. 2021;17:210144.
-
Suehs CM, et al. Am J Respir Crit Care Med. 2021;203(7):871-881. 4. Tran TN, et al. J Allergy Clin Immunol Pract. 2021;9(1):338-346. 5. Tran TN, et al. Eur Respir J. 2020;55(6):1902363. 6. Romão M, et al. J Asthma Allergy. 2022;15:1579-1592.
-
Sher LD, Wechsler ME, Rabe KF, et al. Dupilumab reduces oral corticosteroid use in patients with corticosteroiddependent severe asthma: an analysis of the phase 3, open-label extension TRAVERSE trial. Chest. 2022;162(1):46-55.
-
Rabe KF, Nair P, Brusselle G, et al. Efficacy and safety of dupilumab in glucocorticoiddependent severe asthma. N Engl J Med. 2018;378(26):2475-2485.
-
Brusselle GG, Koppelman GH. Biologic therapies for severe asthma. N Eng J Med. 2022;386(2):157-171.
Abbreviations
EOS: Eosinophils ; FeNO: fractional exhaled nitric oxide levels ; IL: Interleukine ; IgE: immunoglobulines E ; mOCS: maintenance oral corticosteroid ; OCS: oral corticosteroids
Related pages
Page Remission
Expert perspective: Complex type 2 inflammation, refreshingly simple
How to target Type 2 inflammation at the source?
Page Remission
Expert perspective: Complex type 2 inflammation, refreshingly simple
How to target Type 2 inflammation at the source?
MAT-BE-2600609-1.0-22/05/2026